0% found this document useful (0 votes)
23 views1 pageJustification Letter
This health form from Kawayam National High School requires individuals to declare that their household has not been in contact with COVID-19 cases and does not exhibit related symptoms. It emphasizes the importance of truthful information and outlines the protection of personal data under the Data Privacy Act. The form will be destroyed 20 days after completion in accordance with national protocols.
Uploaded by
Tricia GalitCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
23 views1 pageJustification Letter
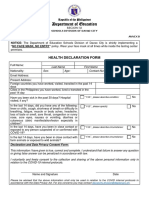
This health form from Kawayam National High School requires individuals to declare that their household has not been in contact with COVID-19 cases and does not exhibit related symptoms. It emphasizes the importance of truthful information and outlines the protection of personal data under the Data Privacy Act. The form will be destroyed 20 days after completion in accordance with national protocols.
Uploaded by
Tricia GalitCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as DOCX, PDF, TXT or read online on Scribd