You might also like
- Valeriano Prince RonnelDocument2 pagesValeriano Prince RonnelPRINCE RONNEL VALERIANONo ratings yet
- STUDENT HEALTH ASSESSMENT FORM (OLFUDocument2 pagesSTUDENT HEALTH ASSESSMENT FORM (OLFUAlex MendozaNo ratings yet
- Health Assessment Form For Student Bais, EvienFrancheskaD.Document2 pagesHealth Assessment Form For Student Bais, EvienFrancheskaD.Evien FrancheskaNo ratings yet
- Health Assessment Form For Student 02Document2 pagesHealth Assessment Form For Student 02Evien FrancheskaNo ratings yet
- Health Assessment Form For Student 02Document2 pagesHealth Assessment Form For Student 02Evien FrancheskaNo ratings yet
- Pneumonia EvaluationDocument3 pagesPneumonia Evaluatione-MedTools50% (2)
- CT3a 2.2 Heart Failure Hypertension Dyslipidemia Reyes WiniDocument14 pagesCT3a 2.2 Heart Failure Hypertension Dyslipidemia Reyes WiniAsylum AllegoryNo ratings yet
- ED RN skills checklistDocument4 pagesED RN skills checklistJohn Carl Angelo EstrellaNo ratings yet
- This Document and The Information Thereon Is The Property of PHINMA Education (Department of Nursing)Document12 pagesThis Document and The Information Thereon Is The Property of PHINMA Education (Department of Nursing)Retiza EllaNo ratings yet
- Skills Checklist (HCA and Mental Health) - Copy (1710)Document2 pagesSkills Checklist (HCA and Mental Health) - Copy (1710)Mohammad Tayyab KhanNo ratings yet
- Medical History FormDocument1 pageMedical History FormCarlos SegoviaNo ratings yet
- Rumah Sakit Umum Yarsi PontianakDocument32 pagesRumah Sakit Umum Yarsi PontianakNabila EdwardNo ratings yet
- Sibayan - Health Assessment FormDocument1 pageSibayan - Health Assessment FormAlberlee SibayanNo ratings yet
- Health Questionnaire: MohamadDocument2 pagesHealth Questionnaire: MohamadMoh AmmNo ratings yet
- Drug Study HIVDocument10 pagesDrug Study HIVAudrie Allyson GabalesNo ratings yet
- Student Health Assessment FormDocument2 pagesStudent Health Assessment FormOrejola, Jonnast P. 2104No ratings yet
- TB Symptom QuestionnaireDocument3 pagesTB Symptom QuestionnaireJayson LeybaNo ratings yet
- Student Health Assessment FormDocument2 pagesStudent Health Assessment FormGelo DizonNo ratings yet
- Haf - Pineda, Aurea MarieDocument1 pageHaf - Pineda, Aurea MarieAurea Marie PinedaNo ratings yet
- Health Declaration FormDocument2 pagesHealth Declaration FormMark Israel DirectoNo ratings yet
- Student Health Assessment FormDocument1 pageStudent Health Assessment FormWonie booNo ratings yet
- Patient Assessment ChecklistDocument2 pagesPatient Assessment ChecklistDaintm AdiNo ratings yet
- Maternal Child Health Nursing Physical Assessment and Labor DiscomfortsDocument18 pagesMaternal Child Health Nursing Physical Assessment and Labor DiscomfortsVanessa Mae Dela CruzNo ratings yet
- Diseases and their symptoms, treatments, and complicationsDocument2 pagesDiseases and their symptoms, treatments, and complicationsCarlos BarreraNo ratings yet
- Student'S Health Assessment Form: Richardson E. InocencioDocument2 pagesStudent'S Health Assessment Form: Richardson E. InocencioJae ChanNo ratings yet
- Health-Assessment-Form-LabongDocument1 pageHealth-Assessment-Form-LabongACMARY ANNE LABONGNo ratings yet
- Medical Declaration 2022 2023Document1 pageMedical Declaration 2022 2023M. YoussefNo ratings yet
- COVID Co-Morbidity Self-DeclarationDocument1 pageCOVID Co-Morbidity Self-Declarationyinka omojesuNo ratings yet
- Living Donor Packet PDF September 2020Document8 pagesLiving Donor Packet PDF September 2020Emilia ColladoNo ratings yet
- A4 Medication Administration and Dosage CalculationDocument47 pagesA4 Medication Administration and Dosage CalculationSHIELOU LOMODNo ratings yet
- Nursing Care of The Client During Labor and DeliveryDocument30 pagesNursing Care of The Client During Labor and DeliveryAnnaverjoy Galvez CuajaoNo ratings yet
- DSMES Intervention Tracking Form (Chart 7)Document1 pageDSMES Intervention Tracking Form (Chart 7)Bryan MorteraNo ratings yet
- Obesity-Ocused Physical Exam: Date - Patient InformationDocument2 pagesObesity-Ocused Physical Exam: Date - Patient InformationDem BertoNo ratings yet
- Cancer Treatment, Going Home After (Let's Talk About... Pediatric Brochure) SpanishDocument4 pagesCancer Treatment, Going Home After (Let's Talk About... Pediatric Brochure) SpanishY GNo ratings yet
- MS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DDocument8 pagesMS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DShawn TejanoNo ratings yet
- OB-GYN Patient History and PEDocument4 pagesOB-GYN Patient History and PEAngelique TongsonNo ratings yet
- BlankDocument2 pagesBlankShyica SalacNo ratings yet
- Vaccine Administration Record (VAR) - Informed Consent For VaccinationDocument2 pagesVaccine Administration Record (VAR) - Informed Consent For VaccinationHilda LunaNo ratings yet
- Reviewer Pharma-Lec FinalsDocument47 pagesReviewer Pharma-Lec FinalsZAIRA MAE MENDERONo ratings yet
- Dicyclomine Drug Study SummaryDocument4 pagesDicyclomine Drug Study SummaryLeslie Lagat PaguioNo ratings yet
- Fundamentals of NursingDocument4 pagesFundamentals of NursingMaricel DuposNo ratings yet
- ROJoson PEP TALK: Abdominal Pain - An OverviewDocument94 pagesROJoson PEP TALK: Abdominal Pain - An OverviewrojosonNo ratings yet
- نسخة نسخة Note 11 Feb 2023 2Document4 pagesنسخة نسخة Note 11 Feb 2023 2Elaf.No ratings yet
- Grade 12 Java Delos Santos Michael JacobDocument2 pagesGrade 12 Java Delos Santos Michael JacobJacob Delos SantosNo ratings yet
- DSMES Intervention Tracking Form (Chart 7) Bryan SignedDocument1 pageDSMES Intervention Tracking Form (Chart 7) Bryan SignedBryan MorteraNo ratings yet
- Immunization Poster LifespanDocument1 pageImmunization Poster Lifespanapi-533830260No ratings yet
- Activity No. 2 - Case Study - Ncp-VillanuevaDocument4 pagesActivity No. 2 - Case Study - Ncp-VillanuevaIrish VillanuevaNo ratings yet
- Handouts Onco Prof. RojasDocument5 pagesHandouts Onco Prof. RojasChallen CulturaNo ratings yet
- Look Under Drugs Affecting Nutritional and Metbolic FunctionDocument1 pageLook Under Drugs Affecting Nutritional and Metbolic FunctionChrissieNo ratings yet
- Antihypertensive MedicationsDocument88 pagesAntihypertensive MedicationsMoxie MacadoNo ratings yet
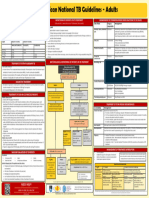
- TB Adult 2017Document1 pageTB Adult 2017zamathefirstNo ratings yet
- Marquez 12d NCP Mod 3Document2 pagesMarquez 12d NCP Mod 3Macy MarquezNo ratings yet
- Risk Assessment FormDocument1 pageRisk Assessment Formncd.bulacanNo ratings yet
- IMCI Patient Assessment FormDocument2 pagesIMCI Patient Assessment FormDa Bondad50% (2)
- Thyroid Crisis and Thyroid Cardiac Disease With Acute Hepatitis ComplicationDocument31 pagesThyroid Crisis and Thyroid Cardiac Disease With Acute Hepatitis ComplicationFuji YantoNo ratings yet
- GE in ChildrenDocument23 pagesGE in ChildrensamiNo ratings yet
- Health Declaration Screening FormDocument1 pageHealth Declaration Screening FormfitchNo ratings yet
- DSMES Assessment Template (Chart 7)Document5 pagesDSMES Assessment Template (Chart 7)Bryan MorteraNo ratings yet
- Brand Management - Kishor Kshirsagar - 17028Document14 pagesBrand Management - Kishor Kshirsagar - 17028kishor kshirsagarNo ratings yet
- The Complete Dysphagia Diet Cookbook:The Ultimate Nutrition Guide For People With Swallowing And Chewing Difficulties With Foodlist, Meal Plan And Nourishing RecipesFrom EverandThe Complete Dysphagia Diet Cookbook:The Ultimate Nutrition Guide For People With Swallowing And Chewing Difficulties With Foodlist, Meal Plan And Nourishing RecipesNo ratings yet
- Ayurveda and Geriatric CareDocument56 pagesAyurveda and Geriatric CareCYBERPHARMNo ratings yet
- COPD-Nutrition-Tips v1.2 LR WM - cv01Document16 pagesCOPD-Nutrition-Tips v1.2 LR WM - cv01Marvin John Surla PegaNo ratings yet
- Respiratory NCLEX Practice Test Part 1: Guillain-Barré SyndromeDocument20 pagesRespiratory NCLEX Practice Test Part 1: Guillain-Barré SyndromeHasan A AsFour100% (2)
- Medicine CBTDocument73 pagesMedicine CBTNadia SalwaniNo ratings yet
- 2021 Mar APEC Agenda Template-TW SGDocument3 pages2021 Mar APEC Agenda Template-TW SGBong Yi LinNo ratings yet
- Usmani 2021 AerosphereDocument12 pagesUsmani 2021 AerosphereRadu CiprianNo ratings yet
- Combined Dental Management of Patients With Medical ConditionsDocument65 pagesCombined Dental Management of Patients With Medical ConditionsJenny WangNo ratings yet
- Textbooks of Pulmonary RehabilitationDocument383 pagesTextbooks of Pulmonary RehabilitationMaghiar Ioana67% (3)
- Common HCC Codes and Diabetes Manifestations SheetDocument2 pagesCommon HCC Codes and Diabetes Manifestations SheetmeikaizenNo ratings yet
- PCCP Leadership and Activities 2014-15Document12 pagesPCCP Leadership and Activities 2014-15Marvel Delos SantosNo ratings yet
- AARC Clinical Practice Guideline: Incentive SpirometryDocument10 pagesAARC Clinical Practice Guideline: Incentive SpirometrytruptimptNo ratings yet
- Drug CardsDocument16 pagesDrug Cardsp_dawg100% (7)
- COPD Exacerbation Management Primary CareDocument1 pageCOPD Exacerbation Management Primary Caremufidah mawaddahNo ratings yet
- Respiratory DiseaseDocument206 pagesRespiratory Diseasemulugetaketema394No ratings yet
- Prelim OncologyDocument10 pagesPrelim OncologyErl D. MelitanteNo ratings yet
- Diet and COPD 2002Document6 pagesDiet and COPD 2002Niar MarhaliNo ratings yet
- Preoperative Evaluation For Non-Cardiac Surgery: AK GhoshDocument6 pagesPreoperative Evaluation For Non-Cardiac Surgery: AK GhoshAshvanee Kumar SharmaNo ratings yet
- Pertanyaan JurnalDocument2 pagesPertanyaan JurnalodivarNo ratings yet
- Alternative Carriers in Dry Powder InhalerDocument9 pagesAlternative Carriers in Dry Powder InhalerApoorva KNo ratings yet
- GINA 2020 Full Report - Final - Wms PDFDocument211 pagesGINA 2020 Full Report - Final - Wms PDFAngelica IpardjoNo ratings yet
- EU CBRN CoE Project 61 - Sound Management of ChemicalsDocument8 pagesEU CBRN CoE Project 61 - Sound Management of ChemicalsTonyo LinaNo ratings yet
- Health 8 Fourth QuarterDocument19 pagesHealth 8 Fourth QuarterAbcde FghijkNo ratings yet
- VentolinDocument13 pagesVentolinFitrah NstNo ratings yet
- NCK Examination Past Pps1,2,3,4-1Document59 pagesNCK Examination Past Pps1,2,3,4-1jimwao100% (1)
- Nursing Practice ConceptDocument19 pagesNursing Practice ConceptpauchanmnlNo ratings yet
- Occupational Lung Diseases: Pneumoconioses and Dust ExposureDocument11 pagesOccupational Lung Diseases: Pneumoconioses and Dust ExposureEMMANUEL BOTSHELONo ratings yet
- Focus Charting 2Document65 pagesFocus Charting 2Ella Caro100% (1)
- Lungs - Facts, Function and Diseases - Live ScienceDocument12 pagesLungs - Facts, Function and Diseases - Live ScienceImtiax LaghariNo ratings yet
- GOLD For COPD Pocket GuideDocument30 pagesGOLD For COPD Pocket Guideraul sinatoNo ratings yet