You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5810)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (346)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cardiac Rehabilitation Assessment FormDocument14 pagesCardiac Rehabilitation Assessment FormCHANDAN RAI100% (2)
- الخلاصه في 23 ورقهDocument23 pagesالخلاصه في 23 ورقهصلاح البازليNo ratings yet
- Summer Training Guide For Pharmacy Students-1Document132 pagesSummer Training Guide For Pharmacy Students-1Rania T. Sabri100% (2)
- Pathogenesis, Diagnosis and Treatment of Rasmussen EncephalitisDocument20 pagesPathogenesis, Diagnosis and Treatment of Rasmussen Encephalitisidno1008No ratings yet
- To Whom It May ConcernDocument1 pageTo Whom It May Concernidno1008100% (1)
- New Drugs For Epilepsy Mangement 1Document48 pagesNew Drugs For Epilepsy Mangement 1idno1008No ratings yet
- EEG1Document13 pagesEEG1idno1008No ratings yet
- Department of NeuromedicineDocument4 pagesDepartment of Neuromedicineidno1008No ratings yet
- Farzana ApuDocument1 pageFarzana Apuidno1008No ratings yet
- Musa IbrahimDocument3 pagesMusa Ibrahimidno1008No ratings yet
- What To Do, When Gbs PT Fails To Respond To TreatmentDocument4 pagesWhat To Do, When Gbs PT Fails To Respond To Treatmentidno1008No ratings yet
- Dr. ShahriarDocument1 pageDr. Shahriaridno1008No ratings yet
- CIDPDocument21 pagesCIDPidno1008No ratings yet
- Daily StarDocument3 pagesDaily Staridno1008No ratings yet
- Activities of Neuromedicine DepartmentDocument2 pagesActivities of Neuromedicine Departmentidno1008No ratings yet
- Admin Protocol AhdDocument1 pageAdmin Protocol Ahdidno1008No ratings yet
- Aseptic MeningitisDocument24 pagesAseptic Meningitisidno1008100% (1)
- StrokesDocument1 pageStrokesidno1008No ratings yet
- Recurrent MeningitisDocument14 pagesRecurrent Meningitisidno1008No ratings yet
- ParkinsonsDocument2 pagesParkinsonsidno1008No ratings yet
- Vestibular Rehabilitation ExercisesDocument1 pageVestibular Rehabilitation Exercisesidno1008No ratings yet
- MigraneDocument1 pageMigraneidno1008No ratings yet
- Neck Exercises1Document3 pagesNeck Exercises1idno1008No ratings yet
- DementiaDocument1 pageDementiaidno1008No ratings yet
- Safety and Efficacy of Statin TherapyDocument13 pagesSafety and Efficacy of Statin TherapyAlexa ArceNo ratings yet
- Open Letter To FDA On Its Response To MRC's Citizen Petition RE The Vascepa SNDADocument56 pagesOpen Letter To FDA On Its Response To MRC's Citizen Petition RE The Vascepa SNDAMedical Research Collaborative, LLCNo ratings yet
- Reference ID: 4109856: 1 Indications and Usage 4 ContraindicationsDocument52 pagesReference ID: 4109856: 1 Indications and Usage 4 Contraindicationsgmsanto7No ratings yet
- Do Lipitor Side Effects Outweigh The Potential Benefits?Document7 pagesDo Lipitor Side Effects Outweigh The Potential Benefits?bigbill138No ratings yet
- Rosuvastatin: Role in Secondary Prevention of Cardiovascular DiseaseDocument5 pagesRosuvastatin: Role in Secondary Prevention of Cardiovascular Diseasenasir uddinNo ratings yet
- Beyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDocument54 pagesBeyond Statins - NEW AHA/ACC Cholesterol Guidelines: Diane Osborn ARNP, CLSDilan GalaryNo ratings yet
- Supralip 160 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)Document8 pagesSupralip 160 MG Film-Coated Tablets - Summary of Product Characteristics (SMPC) - Print Friendly - (Emc)bhavaniNo ratings yet
- Interaction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionDocument5 pagesInteraction Between Amlodipine and Simvastatin in Patients With Hypercholesterolemia and HypertensionSuci Ika PratiwiNo ratings yet
- Stopp Start ToolkitDocument22 pagesStopp Start ToolkitRifky IlhamiNo ratings yet
- Drug Study: Drug Classificati ON Mechanism of Action Rationale Common Side Effects Nursing ConsiderationDocument5 pagesDrug Study: Drug Classificati ON Mechanism of Action Rationale Common Side Effects Nursing ConsiderationMaye ArugayNo ratings yet
- Zocor (Simvastatin)Document3 pagesZocor (Simvastatin)E100% (1)
- The Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainDocument5 pagesThe Pathological Effects of Hyperglycaemia On The Cardiovascular (CV) System and BrainRyzka Izza MayFanyNo ratings yet
- Non Medical Prescribing Using The British National Formulary PDFDocument6 pagesNon Medical Prescribing Using The British National Formulary PDFRyan MwNo ratings yet
- Askep Angina Pectoris Bhs InggrisDocument16 pagesAskep Angina Pectoris Bhs InggrisMillitio ChristiantoroNo ratings yet
- Manuscript - 1716 - 12-TJNPR-2021-M200 Galley Proof CDocument6 pagesManuscript - 1716 - 12-TJNPR-2021-M200 Galley Proof CelisNo ratings yet
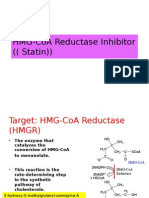
- HMG-CoA Reductase InhibitorDocument10 pagesHMG-CoA Reductase InhibitorGilang Sumiarsih PramanikNo ratings yet
- Essential Notes For The MRCP 3rd PDFDocument613 pagesEssential Notes For The MRCP 3rd PDFnayhtun2471100% (1)
- DiltiazemDocument12 pagesDiltiazemKalpit SahooNo ratings yet
- The American Journal of CardiologyDocument14 pagesThe American Journal of CardiologyDissa AryasanindyaNo ratings yet
- Public Health Perspectives Journal: Christina Ary Yuniarti, RR Sri Ratna Rahayu, Ari YuniastutiDocument10 pagesPublic Health Perspectives Journal: Christina Ary Yuniarti, RR Sri Ratna Rahayu, Ari YuniastutiWildanul HasanahNo ratings yet
- National Institute For Health and Care Excellence Guidelines For Lipid ManagementDocument7 pagesNational Institute For Health and Care Excellence Guidelines For Lipid ManagementSOFIA SANCHEZ GONZALEZNo ratings yet
- Coronary Artery Diseases - Ilham PDocument43 pagesCoronary Artery Diseases - Ilham PKeputrian FKUPNo ratings yet
- Diabetic DyslipidemiaDocument80 pagesDiabetic Dyslipidemiasriworo100% (1)
- Eurheartj Ehw272 FullDocument72 pagesEurheartj Ehw272 FullFabian SanabriaNo ratings yet
- Evidence Based Cardiology 4th EdDocument424 pagesEvidence Based Cardiology 4th EdROGER LUDEÑA SALAZARNo ratings yet
- Improvement Dissolution Rate and Bioavailability of Simvastatin TabletDocument10 pagesImprovement Dissolution Rate and Bioavailability of Simvastatin TabletTaufik Rizki RamdamiNo ratings yet
- Pat Fundies 2016Document18 pagesPat Fundies 2016api-371817203No ratings yet