0% found this document useful (0 votes)
68 views15 pagesMaster List Template
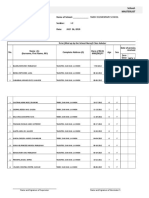
The document is a vaccination consent form for Grade 1 students in Tarlac, Philippines, detailing sections for personal information, vaccination details, and signatures from health officials. It includes spaces for recording the number of vaccines received, used, and unused, as well as health history and consent status. The form is structured to be filled out by both the local health center and the vaccination team.
Uploaded by
Fairy-Lou Hernandez MejiaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd
0% found this document useful (0 votes)
68 views15 pagesMaster List Template
The document is a vaccination consent form for Grade 1 students in Tarlac, Philippines, detailing sections for personal information, vaccination details, and signatures from health officials. It includes spaces for recording the number of vaccines received, used, and unused, as well as health history and consent status. The form is structured to be filled out by both the local health center and the vaccination team.
Uploaded by
Fairy-Lou Hernandez MejiaCopyright
© © All Rights Reserved
We take content rights seriously. If you suspect this is your content, claim it here.
Available Formats
Download as XLSX, PDF, TXT or read online on Scribd