You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- 1141 FullDocument20 pages1141 FullnofiasaridNo ratings yet
- GG 17Document11 pagesGG 17Rahadiyan HadinataNo ratings yet
- ChemoStabilityChart AtoK 14jan2014Document42 pagesChemoStabilityChart AtoK 14jan2014nofiasaridNo ratings yet
- Pharmacokinetics Cephalexin: Dosage Nomograms Impaired: of Cefaclor and For Renal FunctionDocument6 pagesPharmacokinetics Cephalexin: Dosage Nomograms Impaired: of Cefaclor and For Renal FunctionnofiasaridNo ratings yet
- Am. J. Epidemiol. 2010 Risnes Aje - kwq400Document9 pagesAm. J. Epidemiol. 2010 Risnes Aje - kwq400nofiasaridNo ratings yet
- Cefsulodin Pharmacokinetics in Patients With Various Degrees of Renal FunctionDocument5 pagesCefsulodin Pharmacokinetics in Patients With Various Degrees of Renal FunctionnofiasaridNo ratings yet
- Influence of Efflux Transporters On Drug.1Document6 pagesInfluence of Efflux Transporters On Drug.1nofiasaridNo ratings yet
- Cefsulodin Pharmacokinetics in Patients With Various Degrees of Renal FunctionDocument5 pagesCefsulodin Pharmacokinetics in Patients With Various Degrees of Renal FunctionnofiasaridNo ratings yet
- Aac00167-0111 2Document5 pagesAac00167-0111 2nofiasaridNo ratings yet
- Aac00164 0175Document6 pagesAac00164 0175nofiasaridNo ratings yet
- Self Inspection and Quality AuditsDocument12 pagesSelf Inspection and Quality Auditsnofiasarid100% (1)
- Aac00164 0175Document6 pagesAac00164 0175nofiasaridNo ratings yet
- Administration of Indinavir and Low-Dose Ritonavir (800/100 MG Twice Daily) With Food Reduces Nephrotoxic Peak Plasma Levels of IndinavirDocument6 pagesAdministration of Indinavir and Low-Dose Ritonavir (800/100 MG Twice Daily) With Food Reduces Nephrotoxic Peak Plasma Levels of IndinavirnofiasaridNo ratings yet
- Articel About Comparable Pharmacokinetics of Generic Indinavir (Inhibisam) Versus Brand Indinavir (Crixivan) When Boosted With RitonavirDocument4 pagesArticel About Comparable Pharmacokinetics of Generic Indinavir (Inhibisam) Versus Brand Indinavir (Crixivan) When Boosted With RitonavirnofiasaridNo ratings yet
- Pharmacokinetics and Pharmacodynamics of Indinavir With or Without Low-Dose Ritonavir in HIV-infected Thai PatientsDocument8 pagesPharmacokinetics and Pharmacodynamics of Indinavir With or Without Low-Dose Ritonavir in HIV-infected Thai PatientsnofiasaridNo ratings yet
- The Use of Pharmacokinetically Guided Indinavir Dose Reductions in The Management of Indinavir-Associated Renal ToxicityDocument7 pagesThe Use of Pharmacokinetically Guided Indinavir Dose Reductions in The Management of Indinavir-Associated Renal ToxicitynofiasaridNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- IST's - HPVDocument17 pagesIST's - HPVCaio BarbosaNo ratings yet
- TBL 15 V4 - Viral PneumoniaDocument24 pagesTBL 15 V4 - Viral PneumoniaFaysal RafiNo ratings yet
- Bacterial identification chartDocument2 pagesBacterial identification chartKristine PangahinNo ratings yet
- Week 2. Learning Module Prokaryotic vs. Eukaryotic OrganismDocument25 pagesWeek 2. Learning Module Prokaryotic vs. Eukaryotic OrganismFezaret Jerome C.No ratings yet
- Herpes Fact SheetDocument2 pagesHerpes Fact SheetRebecca RichardsonNo ratings yet
- The Animal Rules 1962 MalaysiaDocument11 pagesThe Animal Rules 1962 MalaysiaMelissa GimballNo ratings yet
- SARS PowerpointDocument44 pagesSARS PowerpointXinn Xinn Vanzandt100% (1)
- Dichotomous Key SampleDocument1 pageDichotomous Key SampleGerald ShouNo ratings yet
- Unsafe Abortion Leads to Life-Threating SepsisDocument4 pagesUnsafe Abortion Leads to Life-Threating SepsisHoneylyn100% (1)
- Recurrent Herpes LabialisDocument25 pagesRecurrent Herpes LabialisGarry B GunawanNo ratings yet
- Diagnosis of LeprosyDocument25 pagesDiagnosis of LeprosyjeevamicroNo ratings yet
- Health Phrasal Verbs Fun Activities Games - 12481Document2 pagesHealth Phrasal Verbs Fun Activities Games - 12481Molnár LajosNo ratings yet
- NEMATODESDocument4 pagesNEMATODESAbby VillamuchoNo ratings yet
- Tinciones Especiales DiapathDocument66 pagesTinciones Especiales DiapathZainMalikNo ratings yet
- Michael G. Glasspool FRCS, DO (Auth.) - Atlas of Ophthalmology-Springer Netherlands (1982) PDFDocument117 pagesMichael G. Glasspool FRCS, DO (Auth.) - Atlas of Ophthalmology-Springer Netherlands (1982) PDFInna BujorNo ratings yet
- The Changing Context of Hepatitis D: ReviewDocument12 pagesThe Changing Context of Hepatitis D: ReviewHadi KuriryNo ratings yet
- How To Transmit A Covid-19 VirusDocument2 pagesHow To Transmit A Covid-19 VirusFelica Angelina (P) X.IS.5No ratings yet
- Transparency Concerns Led To Energy Minister Change: Remembering An Uprising, 25 Years OnDocument88 pagesTransparency Concerns Led To Energy Minister Change: Remembering An Uprising, 25 Years OnThe Myanmar TimesNo ratings yet
- Allied Exam Answer Key Errors Matter To CM by Vijay Kumar HeerDocument19 pagesAllied Exam Answer Key Errors Matter To CM by Vijay Kumar HeerVIJAY KUMAR HEERNo ratings yet
- A Case Study of Ankylosing SpondylitisDocument10 pagesA Case Study of Ankylosing SpondylitisVenkatesan VidhyaNo ratings yet
- NCP To NG PneumoniaDocument3 pagesNCP To NG PneumoniaGlenn Asuncion PagaduanNo ratings yet
- Mouthwashes and Their Use in Different Oral ConditionsDocument6 pagesMouthwashes and Their Use in Different Oral ConditionsBagus RahmawanNo ratings yet
- Hepatitis B: DR Tanmay Vyas (DM Hepatology)Document37 pagesHepatitis B: DR Tanmay Vyas (DM Hepatology)Sreekanth VattikondaNo ratings yet
- What Is The Flu? How Is The Flu Spread?Document2 pagesWhat Is The Flu? How Is The Flu Spread?porfirio ruizNo ratings yet
- Thypoid FeverDocument6 pagesThypoid FeverRizki DickyNo ratings yet
- Louis Pasteur (1822-1895)Document12 pagesLouis Pasteur (1822-1895)NercyNo ratings yet
- World of Darkness - Three Shades of NightDocument290 pagesWorld of Darkness - Three Shades of NightBilly Mott86% (7)
- MCQs for ENT: Single Best Answers (SBAsDocument89 pagesMCQs for ENT: Single Best Answers (SBAsMiguel Quispe100% (1)
- Probiotic Activities of Lcr35 in Vitro Adherence To Intestinal Cells and Antimicrobial PropertiesDocument7 pagesProbiotic Activities of Lcr35 in Vitro Adherence To Intestinal Cells and Antimicrobial PropertiesMaria TejedaNo ratings yet
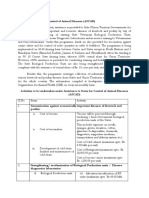
- Assistance To States For Control of Animal Diseases (ASCADDocument6 pagesAssistance To States For Control of Animal Diseases (ASCADMonal DaptardarNo ratings yet