You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Acantholytic Solar Keratosis, M 67, Forehead PDFDocument6 pagesAcantholytic Solar Keratosis, M 67, Forehead PDFDeba P SarmaNo ratings yet
- Acantholytic Bullous DiseaseDocument4 pagesAcantholytic Bullous DiseaseDeba P SarmaNo ratings yet
- Accessory TragusDocument3 pagesAccessory TragusDeba P SarmaNo ratings yet
- Pilar Cyst With CrystalsDocument2 pagesPilar Cyst With CrystalsDeba P SarmaNo ratings yet
- Acantholytic Dermatosis With DyskeratosisDocument11 pagesAcantholytic Dermatosis With DyskeratosisDeba P SarmaNo ratings yet
- Acantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Document3 pagesAcantholytic Bullous Disease (Darier's Disease, Keratosis Follicularis)Deba P SarmaNo ratings yet
- Acantholytic Acanthoma. M 60, ScrotumDocument8 pagesAcantholytic Acanthoma. M 60, ScrotumDeba P SarmaNo ratings yet
- Acantholytic Actinic KeratosisDocument4 pagesAcantholytic Actinic KeratosisDeba P SarmaNo ratings yet
- Balanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Document6 pagesBalanitis Circumscripta Plasmacellularis (Zoon's Balanitis, Plasma Cell Balanitis)Deba P SarmaNo ratings yet
- Results of Search in Google Scholar On 'Deba P Sarma'Document28 pagesResults of Search in Google Scholar On 'Deba P Sarma'Deba P SarmaNo ratings yet
- Xanthogranuloma, M 30, Right ElbowDocument4 pagesXanthogranuloma, M 30, Right ElbowDeba P SarmaNo ratings yet
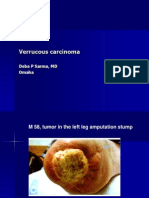
- Verrucous Carcinoma., M 58, Left Leg Amputation StumpDocument7 pagesVerrucous Carcinoma., M 58, Left Leg Amputation StumpDeba P SarmaNo ratings yet
- Xanthogranuloma PPT DSDocument9 pagesXanthogranuloma PPT DSDeba P SarmaNo ratings yet
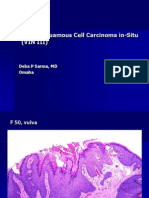
- Vulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDocument6 pagesVulvar Squamous Cell Carcinoma In-Situ (VIN III), F 50, VulvaDeba P SarmaNo ratings yet
- Xanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDocument7 pagesXanthomatous Synovial Cyst (Xanthomatous Ganglion Cyst), M 74, Left PalmDeba P SarmaNo ratings yet
- Verrucous Epidermal Nevus. F 43, ScalpDocument4 pagesVerrucous Epidermal Nevus. F 43, ScalpDeba P SarmaNo ratings yet
- Verrucous Carcinoma of The Foot, M 63, Left FootDocument8 pagesVerrucous Carcinoma of The Foot, M 63, Left FootDeba P Sarma100% (1)
- Verruca Vulgaris., M 22.,PPTDocument2 pagesVerruca Vulgaris., M 22.,PPTDeba P SarmaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Reaction On The 83RD Post Graduate Course On Occupational Health and SafetyDocument1 pageReaction On The 83RD Post Graduate Course On Occupational Health and SafetyEdcelle SabanalNo ratings yet
- Timing Light Schematic or DiagramDocument2 pagesTiming Light Schematic or Diagramprihharmanto antokNo ratings yet
- K 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Document28 pagesK 46 Compact Spinning Machine Brochure 2530-V3 75220 Original English 75220Pradeep JainNo ratings yet
- Why The Sea Is SaltDocument3 pagesWhy The Sea Is SaltVictor CiobanNo ratings yet
- Exercise On Relative ClausesDocument5 pagesExercise On Relative ClausesSAmuel QuinteroNo ratings yet
- Individual Assignment: Prepared By: Tigist WoldesenbetDocument12 pagesIndividual Assignment: Prepared By: Tigist WoldesenbetRobel YacobNo ratings yet
- Design & Evaluation in The Real World: Communicators & Advisory SystemsDocument13 pagesDesign & Evaluation in The Real World: Communicators & Advisory Systemsdivya kalyaniNo ratings yet
- Avatar Legends The Roleplaying Game 1 12Document12 pagesAvatar Legends The Roleplaying Game 1 12azeaze0% (1)
- Iml601 Week 4 AbsDocument69 pagesIml601 Week 4 AbsNur Nazurah NordinNo ratings yet
- Design and Implementation of Computerized Hospital Database MNT SystemDocument13 pagesDesign and Implementation of Computerized Hospital Database MNT SystemOgidiolu Temitope EbenezerNo ratings yet
- (Dr. Mariam) NT40103 AssignmentDocument11 pages(Dr. Mariam) NT40103 AssignmentAhmad Syamil Muhamad ZinNo ratings yet
- Rath'S Lectures: Longevity Related Notes On Vimsottari DasaDocument5 pagesRath'S Lectures: Longevity Related Notes On Vimsottari DasasudhinnnNo ratings yet
- Case StudyDocument3 pagesCase StudyAnqi Liu50% (2)
- Decision Making and Problem Solving & Managing - Gashaw PDFDocument69 pagesDecision Making and Problem Solving & Managing - Gashaw PDFKokebu MekonnenNo ratings yet
- Eor Brochure 2012Document32 pagesEor Brochure 2012Juan Camilo Dangon MolanoNo ratings yet
- Conducting A SeminarDocument17 pagesConducting A SeminarSubhash DhungelNo ratings yet
- The EagleDocument4 pagesThe EagleJunkoNo ratings yet
- RECAP Lecture 7: FA of EVEN EVEN, FA Corresponding To Finite Languages (Using Both Methods), Transition GraphsDocument23 pagesRECAP Lecture 7: FA of EVEN EVEN, FA Corresponding To Finite Languages (Using Both Methods), Transition GraphsMuhammad EahteshamNo ratings yet
- Oscar Characterization TemplateDocument3 pagesOscar Characterization Templatemqs786No ratings yet
- He Didnt Die in Vain - Take No GloryDocument2 pagesHe Didnt Die in Vain - Take No GloryDagaerag Law OfficeNo ratings yet
- People V Galano, Caubang v. PeopleDocument2 pagesPeople V Galano, Caubang v. PeopleHermay Banario50% (2)
- F07 hw07Document2 pagesF07 hw07rahulNo ratings yet
- Procedures: Step 1 Freeze or Restrain The Suspect/sDocument5 pagesProcedures: Step 1 Freeze or Restrain The Suspect/sRgenieDictadoNo ratings yet
- Module 4 Business EthicsDocument4 pagesModule 4 Business EthicsddddddaaaaeeeeNo ratings yet
- BattleRope Ebook FinalDocument38 pagesBattleRope Ebook FinalAnthony Dinicolantonio100% (1)
- 11 Chemistry NcertSolutions Chapter 2 ExercisesDocument54 pages11 Chemistry NcertSolutions Chapter 2 ExercisesGeeteshGuptaNo ratings yet
- Magtajas vs. PryceDocument3 pagesMagtajas vs. PryceRoyce PedemonteNo ratings yet
- Aleister Crowley Astrological Chart - A Service For Members of Our GroupDocument22 pagesAleister Crowley Astrological Chart - A Service For Members of Our GroupMysticalgod Uidet100% (3)
- SKZ TrackDocument6 pagesSKZ TrackOliviaNo ratings yet
- Network Firewall SecurityDocument133 pagesNetwork Firewall Securitysagar323No ratings yet