You might also like
- Thrombosis and Bleeding Disorders: Theory and MethodsFrom EverandThrombosis and Bleeding Disorders: Theory and MethodsNils U. BangRating: 2 out of 5 stars2/5 (1)
- Parameters of Automated Cell Counter Automation in Hematology Laboratory and CBC Via Automated Blood AnalyzerDocument40 pagesParameters of Automated Cell Counter Automation in Hematology Laboratory and CBC Via Automated Blood AnalyzerArslan Arshad100% (1)
- Essentials of ABO -Rh Grouping and Compatibility Testing: Theoretical Aspects and Practical ApplicationFrom EverandEssentials of ABO -Rh Grouping and Compatibility Testing: Theoretical Aspects and Practical ApplicationRating: 5 out of 5 stars5/5 (1)
- Laboratory Hematology PracticeFrom EverandLaboratory Hematology PracticeKandice Kottke-MarchantRating: 5 out of 5 stars5/5 (1)
- Total Leukocyte Count by HemocytometerDocument4 pagesTotal Leukocyte Count by HemocytometerMalkish RajkumarNo ratings yet
- The Notes On Histochemical StainsDocument125 pagesThe Notes On Histochemical StainsDr Joswin Dsa67% (3)
- Bone Marrow Biopsy TechniquesDocument47 pagesBone Marrow Biopsy Techniquesludiegues752No ratings yet
- Paps SmearDocument51 pagesPaps SmearCatherine MerillenoNo ratings yet
- Prepartion of Blood Smear Hematology PresentationDocument44 pagesPrepartion of Blood Smear Hematology PresentationArslan ArshadNo ratings yet
- Cell BlockDocument25 pagesCell BlockD BNo ratings yet
- Tissue ProcessingDocument20 pagesTissue ProcessingUsman AkramNo ratings yet
- Special StainsDocument10 pagesSpecial Stainsjgpd2000100% (1)
- Heme Quiz 1-3Document14 pagesHeme Quiz 1-3Søren KierkegaardNo ratings yet
- Histopathology InstrumentsDocument6 pagesHistopathology InstrumentsLawrence LeeNo ratings yet
- Histopathologic TechniquesDocument22 pagesHistopathologic TechniquesRomie SolacitoNo ratings yet
- Histopathology Chapter 4Document108 pagesHistopathology Chapter 4Zelalem Dejazmach100% (1)
- Peripheral Blood Smear and HistologyDocument26 pagesPeripheral Blood Smear and Histologystudent2013No ratings yet
- Metodos Citodiagnostico MERCKDocument44 pagesMetodos Citodiagnostico MERCKGregorio De Las CasasNo ratings yet
- Histopathology Chapter 2Document141 pagesHistopathology Chapter 2Zelalem Dejazmach100% (2)
- Blood Smear ExaminationDocument65 pagesBlood Smear Examinationqlephon100% (2)
- Special StainDocument45 pagesSpecial StainJerry TurtleNo ratings yet
- Microtomy Paraffin SectionDocument36 pagesMicrotomy Paraffin Sectiondante220No ratings yet
- Hem Lab3 Blood Smears F10Document10 pagesHem Lab3 Blood Smears F10Luke Hsu0% (1)
- CBC Automated AnalyzerDocument55 pagesCBC Automated AnalyzerfaizNo ratings yet
- Blood Bank ProceduresDocument33 pagesBlood Bank Procedures99noname100% (1)
- Basic Haematology: Practical ManualDocument49 pagesBasic Haematology: Practical ManualNipun Shamika100% (1)
- Special Stains PDFDocument58 pagesSpecial Stains PDFmiguel gaquitNo ratings yet
- HISTOPATHOLOGIC AND CYTOLOGIC TECHNIQUES LEC Module 2Document14 pagesHISTOPATHOLOGIC AND CYTOLOGIC TECHNIQUES LEC Module 2Clair TugnaNo ratings yet
- Special Stains in Histopathology: Movat'S Pentachrome StainDocument27 pagesSpecial Stains in Histopathology: Movat'S Pentachrome StainambadepravinNo ratings yet
- Respiratory Cytology: DR Mohammed Shahin, JR (Academic), Dept of Pathology & Lab Medicine, AIIMS BhubaneswarDocument62 pagesRespiratory Cytology: DR Mohammed Shahin, JR (Academic), Dept of Pathology & Lab Medicine, AIIMS BhubaneswarShruthi N.RNo ratings yet
- Tissue ProcessingDocument31 pagesTissue ProcessingZia Ashraf ChaudharyNo ratings yet
- Preparation and Staining Methods For Blood and Bone Marrow FilmsDocument7 pagesPreparation and Staining Methods For Blood and Bone Marrow Filmsادم PrabowoNo ratings yet
- Introduction To Histopathology and CytologyDocument25 pagesIntroduction To Histopathology and CytologyVinayNo ratings yet
- Microtome and Micro To My WordDocument12 pagesMicrotome and Micro To My WordKaran KapoorNo ratings yet
- Pranab Dey - Diagnostic CytologyDocument1 pagePranab Dey - Diagnostic CytologyJose SirittNo ratings yet
- Seminar On Tissue Processing AsDocument49 pagesSeminar On Tissue Processing AsDrPradeep Singh Khanchi100% (1)
- Introduction To HistologyDocument32 pagesIntroduction To HistologyPushparaj ShettyNo ratings yet
- Shandon Finesse Microtome Series: - Features Models Ranging FromDocument12 pagesShandon Finesse Microtome Series: - Features Models Ranging FromVer BautistaNo ratings yet
- Hemocue ManualDocument5 pagesHemocue ManualDhanjit HaloiNo ratings yet
- Blood Film Preparation and Staining Procedures: Erend OuwenDocument7 pagesBlood Film Preparation and Staining Procedures: Erend OuwenSuresh Kumar RamanathanNo ratings yet
- SPECIMEN HANDLING GUIDELINE CorrectedDocument90 pagesSPECIMEN HANDLING GUIDELINE CorrectedDavindu AnushkaNo ratings yet
- Lesson 25 PDFDocument7 pagesLesson 25 PDFSeby SebastianNo ratings yet
- BleedingTime ClottingTimeDocument19 pagesBleedingTime ClottingTimeRamadan PhysiologyNo ratings yet
- PMLS HistopathologyDocument20 pagesPMLS HistopathologyTrixie Cyrah100% (1)
- Blood Smear PreparationDocument125 pagesBlood Smear PreparationKim RuizNo ratings yet
- An Introduction To Routine and Special StainingDocument13 pagesAn Introduction To Routine and Special StainingBadiu ElenaNo ratings yet
- Automation in Clinical ChemistryDocument20 pagesAutomation in Clinical Chemistryakongke20No ratings yet
- Pap StainingDocument2 pagesPap StainingDrManish KumarNo ratings yet
- HE StainDocument2 pagesHE Stainthy100% (2)
- Special TopicsDocument8 pagesSpecial Topicskatherine ruizNo ratings yet
- Hematoxylin and Eosin StainingDocument6 pagesHematoxylin and Eosin StainingRaja Sharma100% (1)
- Performance Rubrics For EtsDocument2 pagesPerformance Rubrics For EtsKim G. SarongNo ratings yet
- Cytological TechniquesDocument4 pagesCytological TechniquesJamie100% (1)
- Relevance of Serum Tumor MarkersDocument25 pagesRelevance of Serum Tumor MarkersDrPawan KirtaniNo ratings yet
- 04 Clinical PathologyDocument73 pages04 Clinical PathologyNabee Azeez0% (3)
- Module 19 - Routine and Special Tissue Processing in HistopathologyDocument100 pagesModule 19 - Routine and Special Tissue Processing in Histopathologyhot silogNo ratings yet
- 6.1.3 Quality Control of Blood ComponentsDocument4 pages6.1.3 Quality Control of Blood ComponentsBALAJINo ratings yet
- Liver AbscessDocument14 pagesLiver AbscessMariaOeiNo ratings yet
- "Traditional" Exegeses of Q 4:34Document15 pages"Traditional" Exegeses of Q 4:34kiedd_04No ratings yet
- From The Bodies of Bees Classical and Christian Echoes in Surah Al-NahlDocument25 pagesFrom The Bodies of Bees Classical and Christian Echoes in Surah Al-Nahlkiedd_04No ratings yet
- Odors of Santity Distinctions of The Holy in Early Christianity and IslamDocument13 pagesOdors of Santity Distinctions of The Holy in Early Christianity and Islamkiedd_04100% (1)
- The Place For Others in IslamDocument27 pagesThe Place For Others in Islamkiedd_04No ratings yet
- Iklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012Document2 pagesIklan Jabatan Pengajian Tinggi (Permohonan Kemasukan Tevt & Ilka) Sesi 2011/2012kiedd_04No ratings yet
- Cell PhysiologyDocument61 pagesCell Physiologykiedd_04100% (4)
- Refleks ArcsDocument34 pagesRefleks Arcskiedd_04100% (1)
- Microbiology Colour Plate No.7Document1 pageMicrobiology Colour Plate No.7kiedd_04No ratings yet
- Microbiology Colour Plate No.8Document1 pageMicrobiology Colour Plate No.8kiedd_04No ratings yet
- Fadhilat Surah at TakwirDocument1 pageFadhilat Surah at Takwirkiedd_04No ratings yet
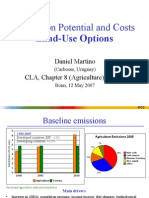
- Mitigation Potential and Costs Land-Use OptionsDocument9 pagesMitigation Potential and Costs Land-Use Optionskiedd_04No ratings yet
- SYNAPSEDocument35 pagesSYNAPSEkiedd_04100% (3)
- Microbiology Colour Plate No.9Document1 pageMicrobiology Colour Plate No.9kiedd_04No ratings yet
- Microbiology Colour Plate No.4Document1 pageMicrobiology Colour Plate No.4kiedd_04No ratings yet
- Microbiology Colour Plate No.6Document1 pageMicrobiology Colour Plate No.6kiedd_04No ratings yet
- API® CoryneDocument4 pagesAPI® Corynekiedd_04No ratings yet
- Microbiology Colour Plate No.1Document1 pageMicrobiology Colour Plate No.1kiedd_04No ratings yet
- Microbiology Colour Plate No.5Document1 pageMicrobiology Colour Plate No.5kiedd_04No ratings yet
- Microbiology Colour Plate No.3Document1 pageMicrobiology Colour Plate No.3kiedd_04No ratings yet
- Philosophical Consolation in Christianity and Islam Boethious and Al-KindiDocument10 pagesPhilosophical Consolation in Christianity and Islam Boethious and Al-Kindikiedd_04No ratings yet
- Mitigation of Climate ChangeDocument41 pagesMitigation of Climate Changekiedd_04No ratings yet
- Microbiology Colour Plate No.2Document1 pageMicrobiology Colour Plate No.2kiedd_04No ratings yet
- Diagram of Classification of EnterobacteriaDocument1 pageDiagram of Classification of Enterobacteriakiedd_04100% (1)
- Carnitine DeficiencyDocument21 pagesCarnitine Deficiencykiedd_04100% (1)
- Mitigation of Climate ChangeDocument25 pagesMitigation of Climate Changekiedd_04No ratings yet
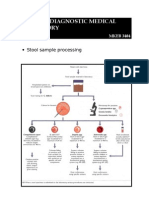
- Stool Sample ProcessingDocument1 pageStool Sample Processingkiedd_04No ratings yet
- Oxidase TestDocument1 pageOxidase Testkiedd_04100% (1)
- Advance Diagnostic Medical Laboratory: The AP 20E® For Identification of BacteriaDocument1 pageAdvance Diagnostic Medical Laboratory: The AP 20E® For Identification of Bacteriakiedd_04100% (1)