You might also like
- Stroke in ChildrenDocument38 pagesStroke in ChildrenberthagabrielNo ratings yet
- Management of Ischemic Stroke in Resource-Limited SettingsDocument34 pagesManagement of Ischemic Stroke in Resource-Limited SettingsericNo ratings yet
- Ern MRCPCHDocument24 pagesErn MRCPCHPasTestBooksNo ratings yet
- Pediatric Stroke: Last Updated by Lindsay Pagano Summer 2013Document9 pagesPediatric Stroke: Last Updated by Lindsay Pagano Summer 2013Khaled GharaibehNo ratings yet
- 4 - Stroke FinalDocument74 pages4 - Stroke FinalSamir SkejicNo ratings yet
- HemiparesisDocument35 pagesHemiparesisIsabela IacobNo ratings yet
- 6 Hemorrhagic StrokeDocument54 pages6 Hemorrhagic StrokeErwinNo ratings yet
- Neuro Case PresentationsDocument25 pagesNeuro Case PresentationsTSunamiNo ratings yet
- Pediatric Trauma AssessmentDocument36 pagesPediatric Trauma AssessmentAbdulrahman Y. SabbaghNo ratings yet
- Diagnosis and Management of Acute StrokeDocument74 pagesDiagnosis and Management of Acute StrokeDonnaBells Hermo Labaniego100% (2)
- CNS M1 Lecture Slides Compiled, DR OsaiDocument185 pagesCNS M1 Lecture Slides Compiled, DR OsaiMusaNo ratings yet
- Dr. A. Ramcharan's Firm Thursday 31 Match 2011Document56 pagesDr. A. Ramcharan's Firm Thursday 31 Match 2011Ronald ChongNo ratings yet
- Understanding Stroke: Causes, Symptoms, Treatment and PreventionDocument16 pagesUnderstanding Stroke: Causes, Symptoms, Treatment and PreventionTith SeavmeyNo ratings yet
- Stroke SyndromeDocument22 pagesStroke Syndromedark15297No ratings yet
- Cerebrovascular Accident in B-Thalassemia Major (B-TM) and B-Thalassemia Intermedia (b-TI)Document3 pagesCerebrovascular Accident in B-Thalassemia Major (B-TM) and B-Thalassemia Intermedia (b-TI)Ni Wayan Ana PsNo ratings yet
- Decompressive Hemicraniectomy and DuroplastyDocument5 pagesDecompressive Hemicraniectomy and DuroplastyAmy NilifdaNo ratings yet
- Cyanotic Congenital Heart DiseasesDocument25 pagesCyanotic Congenital Heart DiseasesAlvin OmondiNo ratings yet
- Nursing Intervention Synthesis/Patient Summary Events Leading To Admission (ER, Direct Admit, Transfer From Another Facility)Document21 pagesNursing Intervention Synthesis/Patient Summary Events Leading To Admission (ER, Direct Admit, Transfer From Another Facility)api-281841077No ratings yet
- Cerebral Sinus ThrombosisDocument23 pagesCerebral Sinus ThrombosisHerinanda Fahmy FahlevieNo ratings yet
- Neonatal EncephalopathyDocument28 pagesNeonatal EncephalopathyRawabi rawabi1997No ratings yet
- The Golden Hour of Acute Ischemic StrokeDocument22 pagesThe Golden Hour of Acute Ischemic StrokeGiao MauNo ratings yet
- Dr. Farin's Grand Round Presentation 31.09.23Document75 pagesDr. Farin's Grand Round Presentation 31.09.23Anika TasnimNo ratings yet
- CVADocument4 pagesCVACloyd Marvin Pajas SegundoNo ratings yet
- 28b- EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020Document8 pages28b- EMRCOG SUMMARY - STROKE IN PREGNANCY - TOG 2020saeed hasan saeedNo ratings yet
- Pedia TriDocument4 pagesPedia TriDIdit FAjar NUgrohoNo ratings yet
- 9, CHF BestDocument43 pages9, CHF BestauNo ratings yet
- Patfall2015 Msii AnjouligerezDocument26 pagesPatfall2015 Msii Anjouligerezapi-325112936No ratings yet
- Odia Tetralogy of FallotDocument25 pagesOdia Tetralogy of Fallotvictorjonathan567No ratings yet
- Grand Case: Submitted ToDocument67 pagesGrand Case: Submitted ToPam Romero0% (1)
- N Eonatal Cardiac Tumor - Case ReportDocument20 pagesN Eonatal Cardiac Tumor - Case ReportmirelasiminelNo ratings yet
- 2019 Enls For ApacvsnnnnnnDocument46 pages2019 Enls For ApacvsnnnnnnAhmed ElshewiNo ratings yet
- Strokes CaseDocument32 pagesStrokes CaseMNo ratings yet
- Pedia SGD NICUDocument62 pagesPedia SGD NICUJAIRISH YZABELLE SALVADORNo ratings yet
- Hypoplastic Left Heart Syndrome - Group ProjectDocument24 pagesHypoplastic Left Heart Syndrome - Group Projectapi-301611629No ratings yet
- Reumato and EndocrineDocument106 pagesReumato and Endocrinehasanatiya41No ratings yet
- Clinical Judgement Exam 2 Study GuideDocument15 pagesClinical Judgement Exam 2 Study GuideAlexa WolffNo ratings yet
- MR - Tn. SDocument20 pagesMR - Tn. SyudistiraanwarNo ratings yet
- Saving Lives Through Trauma CareDocument60 pagesSaving Lives Through Trauma CareSweetcharmed GoNo ratings yet
- Pediatric Trauma: Presented By: Erwin MaulanaDocument39 pagesPediatric Trauma: Presented By: Erwin Maulanaadliah zahiraNo ratings yet
- STROKE RISK FACTORSDocument16 pagesSTROKE RISK FACTORSEmuelle GanNo ratings yet
- 4th Problem Emergency Medicine Group 1Document82 pages4th Problem Emergency Medicine Group 1Jonathan TandajuNo ratings yet
- Stroke PreventionDocument8 pagesStroke PreventionjaanhoneyNo ratings yet
- Clinical Challenges of In-Hospital StrokesDocument57 pagesClinical Challenges of In-Hospital StrokesRizky DimasaputraNo ratings yet
- Archer USMLE Step 3 Question BankDocument116 pagesArcher USMLE Step 3 Question Bankrolpf garri33% (3)
- Megacode 2Document3 pagesMegacode 2JILL ANGELESNo ratings yet
- Approach To A Child With Congenital Heart DiseaseDocument31 pagesApproach To A Child With Congenital Heart DiseaseMUHAMMAD DANIAL BIN HASAN FPSKNo ratings yet
- Patent Ductus ArteriosusDocument4 pagesPatent Ductus ArteriosusseigelysticNo ratings yet
- The Pathophysiology of Ischemic Strokes Is Widely Known. Ischemic Strokes Are TheDocument7 pagesThe Pathophysiology of Ischemic Strokes Is Widely Known. Ischemic Strokes Are Theprnczb13No ratings yet
- Clin Cardiology CasesDocument34 pagesClin Cardiology CasesSunny Singh0% (1)
- EBSTEIN'S ANOMALY Dhini - Maju 17 Juli 2014Document29 pagesEBSTEIN'S ANOMALY Dhini - Maju 17 Juli 2014Azizi PranokoNo ratings yet
- Introduction To Clinical Medicine (ICM) : Case Studies Neurologic DisordersDocument142 pagesIntroduction To Clinical Medicine (ICM) : Case Studies Neurologic DisordersomarNo ratings yet
- Stroke by Dr. AM IyagbaDocument44 pagesStroke by Dr. AM IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Ischemic StrokeDocument20 pagesIschemic StrokeMargaret BaleNo ratings yet
- StrokeDocument55 pagesStrokeOgechi Grace OkoliNo ratings yet
- Congestive Cardiac Failure by NeetaDocument26 pagesCongestive Cardiac Failure by NeetaNeeta AnandaNo ratings yet
- LeukemiaDocument22 pagesLeukemiaPraveen AbhimanyuNo ratings yet
- Hematology 101: Hematology/Oncology PG 1 of 11Document12 pagesHematology 101: Hematology/Oncology PG 1 of 11esther100% (1)
- T T A S: Hrombolytic Herapy in Cute TrokeDocument3 pagesT T A S: Hrombolytic Herapy in Cute TrokevivinNo ratings yet
- Nurse Practitioner Board ReviewFrom EverandNurse Practitioner Board ReviewRating: 5 out of 5 stars5/5 (1)
- Register Harian Apotik 1Document10 pagesRegister Harian Apotik 1muslaeniNo ratings yet
- International Journal of Surgery: Hasanin Al Chalabi, John Larkin, Brian Mehigan, Paul MccormickDocument10 pagesInternational Journal of Surgery: Hasanin Al Chalabi, John Larkin, Brian Mehigan, Paul Mccormickfranco sumolangNo ratings yet
- Digital Drugs An Anatomy of New Medicines PDFDocument27 pagesDigital Drugs An Anatomy of New Medicines PDFshraddha5jNo ratings yet
- Psyche A AkDocument21 pagesPsyche A AkSamuel John SaludezNo ratings yet
- BLUEBIRD (Some Part)Document17 pagesBLUEBIRD (Some Part)Mushtaq RahiNo ratings yet
- DapusDocument2 pagesDapusRismitha AndiniNo ratings yet
- Template - Case Report ArticleDocument4 pagesTemplate - Case Report Articlegerald randyNo ratings yet
- ASSESSMENT DIAGNOSIS PLANNING EVALUATIONDocument2 pagesASSESSMENT DIAGNOSIS PLANNING EVALUATIONJiraGonzalesNo ratings yet
- Ocular Injuries and EmergenciesDocument60 pagesOcular Injuries and Emergenciesarnol3090100% (1)
- MCQ Manual - SCFHSDocument75 pagesMCQ Manual - SCFHSferdinand bolayog0% (3)
- Hotel Spa and Wellness Services in Crete: A Marketing AnalysisDocument6 pagesHotel Spa and Wellness Services in Crete: A Marketing AnalysisestherNo ratings yet
- A Study On Moringa Oleifera Leaves As A Supplement To West African Weaning Foods BA - Kayi - Kristina - KoueviDocument72 pagesA Study On Moringa Oleifera Leaves As A Supplement To West African Weaning Foods BA - Kayi - Kristina - KoueviNutri MoringaNo ratings yet
- Oral Findings and Diagnosis of Systemic Lupus ErythematosusDocument6 pagesOral Findings and Diagnosis of Systemic Lupus ErythematosusArditya Dwi YudistiraNo ratings yet
- Editorial Letter: ﺪﻠﺠﻣ 1 دﺪﻋ 3 - 2004 - Volume 1-N°3, 2004Document141 pagesEditorial Letter: ﺪﻠﺠﻣ 1 دﺪﻋ 3 - 2004 - Volume 1-N°3, 2004CH Karim100% (1)
- Bioconned Water Magnetic Far Infrared New AgeDocument159 pagesBioconned Water Magnetic Far Infrared New AgeFrancis Lobo100% (1)
- Deleuze and Psychology PhilosophicalDocument4 pagesDeleuze and Psychology PhilosophicalVissente TapiaNo ratings yet
- A Complete Healthcare System: MaccabiDocument30 pagesA Complete Healthcare System: MaccabiEnglishAccessibilityNo ratings yet
- University of Eastern Philippines: University Town, Northern SamarDocument5 pagesUniversity of Eastern Philippines: University Town, Northern SamarJane MinNo ratings yet
- Exfoliative DermatitisDocument7 pagesExfoliative DermatitisRidyah Ning TyasNo ratings yet
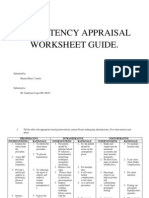
- Competency Appraisal Worksheet Guide (Final)Document10 pagesCompetency Appraisal Worksheet Guide (Final)Shan JanoloNo ratings yet
- Qtsoi Concept MapDocument5 pagesQtsoi Concept MapGenella BabantoNo ratings yet
- Derm CodingDocument8 pagesDerm CodingVinay100% (1)
- R ChopDocument6 pagesR Chopจีทีเอส สุรเชษฐNo ratings yet
- Waste ManagementDocument75 pagesWaste ManagementGururaj Dafale100% (1)
- "Monograph Eating Disorders": StudentDocument12 pages"Monograph Eating Disorders": StudentTeffy NeyraNo ratings yet
- Lower Back Pain SOAP NotesDocument14 pagesLower Back Pain SOAP NotesNorhuzmaira Mohd RofaeiNo ratings yet
- Living With Depression & Coping StrategiesDocument20 pagesLiving With Depression & Coping StrategiesnatasharfNo ratings yet
- Retrospective Study of Cholangiocarcinomas Diagnosed in The Hospital of Fuenlabrada in The Period 20062016Document3 pagesRetrospective Study of Cholangiocarcinomas Diagnosed in The Hospital of Fuenlabrada in The Period 20062016Riya CassendraNo ratings yet
- Otago Exercise ProgrammeDocument71 pagesOtago Exercise Programmesavvy_as_98-1100% (1)
- Management of Clinical Wastes in Malaysia 2 0Document29 pagesManagement of Clinical Wastes in Malaysia 2 0jun005No ratings yet