You might also like
- English For NursingDocument16 pagesEnglish For NursingMaria Apostu StylesNo ratings yet
- Jameswaslaski Pelvicstabilization Uploadable VersionDocument12 pagesJameswaslaski Pelvicstabilization Uploadable VersionMarco PMTNo ratings yet
- Design and Development of C-Arm MachineDocument10 pagesDesign and Development of C-Arm MachineTamilandaNo ratings yet
- Lucrare de Disertatie Satisfactia SexualaDocument100 pagesLucrare de Disertatie Satisfactia Sexualamklogistica106100% (1)
- Planned Parenthood Response To DHHDocument5 pagesPlanned Parenthood Response To DHHKevin LittenNo ratings yet
- Primary Open Angle GlauDocument21 pagesPrimary Open Angle GlauwildaNo ratings yet
- Glaucoma: Consultant OphthalmologistDocument45 pagesGlaucoma: Consultant OphthalmologistGladys MainaNo ratings yet
- GLAUKOMADocument47 pagesGLAUKOMARahma GhnNo ratings yet
- Double Vision / Diplopia: Dr. R. Handoko Pratomo, SPMDocument94 pagesDouble Vision / Diplopia: Dr. R. Handoko Pratomo, SPMNefri TiawarmanNo ratings yet
- Glaucoma & CataractDocument53 pagesGlaucoma & CataractBenita100% (1)
- Degenerative MyopiaDocument53 pagesDegenerative MyopiaNiloy BasakNo ratings yet
- 30secondary GlaucomasDocument15 pages30secondary GlaucomasShari' Si WahyuNo ratings yet
- Retinal Disorders Med VDocument66 pagesRetinal Disorders Med Vhenok birukNo ratings yet
- 30secondary GlaucomasDocument19 pages30secondary GlaucomasShari' Si WahyuNo ratings yet
- Diseases of Orbit: Yang Wei Ophthalmology Department in Affiliated Hospital of Southwest Medical UniversityDocument44 pagesDiseases of Orbit: Yang Wei Ophthalmology Department in Affiliated Hospital of Southwest Medical UniversityIhsan HanifNo ratings yet
- Coats, Eales, Anemia, Lukemia, SC RetinopathyDocument81 pagesCoats, Eales, Anemia, Lukemia, SC RetinopathydryashhadaNo ratings yet
- Mira Ophth NotesDocument27 pagesMira Ophth NotesMorticia AddamsNo ratings yet
- Diabetic RetinopathyDocument101 pagesDiabetic RetinopathyMohiuddin AhmedNo ratings yet
- Glaucoma PresentationDocument57 pagesGlaucoma PresentationIshak Izhar100% (1)
- TRABECULECTOMY Complications FinalDocument31 pagesTRABECULECTOMY Complications FinalalfarizyjefryNo ratings yet
- Atrofia Nervului OpticDocument23 pagesAtrofia Nervului OpticScerbatiuc CristinaNo ratings yet
- PterygiumDocument40 pagesPterygiumKhurram ChauhanNo ratings yet
- PSSS Mata Merah Visus Menurun PerlahanDocument44 pagesPSSS Mata Merah Visus Menurun PerlahandeyshieNo ratings yet
- Cataract: Done by Mo3taz Abu Rabiah A7mad LubaniDocument46 pagesCataract: Done by Mo3taz Abu Rabiah A7mad LubaniMaxwell C Jay KafwaniNo ratings yet
- Secondary Angle Closure GlaucomaDocument35 pagesSecondary Angle Closure GlaucomaAndriati NadhilaNo ratings yet
- Objective of Eye SurgeryDocument51 pagesObjective of Eye SurgeryMuntazir Mehdi Al HassaniNo ratings yet
- Management of CataractDocument28 pagesManagement of CataractMicah JatauNo ratings yet
- Glaucoma & Retinal Detachment-1Document29 pagesGlaucoma & Retinal Detachment-1Priya bhattiNo ratings yet
- OphthalmologyDocument55 pagesOphthalmologyapi-19916399100% (3)
- Cataract: Done by Jony MallikDocument46 pagesCataract: Done by Jony MallikAlfa Suryani ArdliNo ratings yet
- 35 Golden Eye RulesDocument7 pages35 Golden Eye RulesJethro WuNo ratings yet
- Cataracts 1Document18 pagesCataracts 1Hno Joseph MulahNo ratings yet
- Cours CataracteDocument42 pagesCours Cataracteroslane98No ratings yet
- Eye Department Queen Elizabeth HospitalDocument43 pagesEye Department Queen Elizabeth Hospitalarnol3090No ratings yet
- Presentation 2Document57 pagesPresentation 2medhanit anjuloNo ratings yet
- Ent Lesson 8Document45 pagesEnt Lesson 8favourednancie9No ratings yet
- HYPERMETROPIA and Myopia PDFDocument55 pagesHYPERMETROPIA and Myopia PDFDrashti ChudasamaNo ratings yet
- Diskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanDocument73 pagesDiskusi Topik - Ali Mustagi - Mata Normal Visus Turun PerlahanalimustagialgiNo ratings yet
- 30secondary GlaucomasDocument9 pages30secondary GlaucomasWahyu FajarNo ratings yet
- 30secondary GlaucomasDocument9 pages30secondary GlaucomasArtha CimutNo ratings yet
- Vitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkiDocument45 pagesVitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkitusuksedotanNo ratings yet
- Screenshot 2023-07-18 at 14.56.31Document146 pagesScreenshot 2023-07-18 at 14.56.31MOHIT SHARMANo ratings yet
- Ocular Trauma Dr. As-Ali 2 OktoberDocument61 pagesOcular Trauma Dr. As-Ali 2 OktoberYama Piniel FrimantamaNo ratings yet
- Age Related Macular Degeneration: Roshni Agrawal First Year MD ResidentDocument70 pagesAge Related Macular Degeneration: Roshni Agrawal First Year MD ResidentSriniwasNo ratings yet
- Vision Impairment 1Document59 pagesVision Impairment 1122ritik goyalNo ratings yet
- Ophthalmology EmergenciesDocument60 pagesOphthalmology Emergenciesasraf amirullahNo ratings yet
- 22 Optic Disc Evaluation IN GlaucomaDocument49 pages22 Optic Disc Evaluation IN Glaucomapriti089No ratings yet
- Ocular SarcoidosisDocument48 pagesOcular SarcoidosisFabsNo ratings yet
- Glaukoma: Dr. Mandiri Nindiasari, SPM, MSCDocument59 pagesGlaukoma: Dr. Mandiri Nindiasari, SPM, MSCfebienaNo ratings yet
- Congenital Glaucoma FinalDocument48 pagesCongenital Glaucoma FinalMona MohammedNo ratings yet
- Orbit and Lacrimal System 1Document45 pagesOrbit and Lacrimal System 1Йеша Маниш МираниNo ratings yet
- GlaucomaDocument27 pagesGlaucomaEvita PrinceNo ratings yet
- Retina AnswersDocument5 pagesRetina AnswersKhushal Khan KakarNo ratings yet
- Diabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeDocument63 pagesDiabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeNear DeathNo ratings yet
- Vitreo Retinal DisordersDocument47 pagesVitreo Retinal DisordersTabreez KhanNo ratings yet
- Retinal Dystrophies & DegenerationsDocument72 pagesRetinal Dystrophies & Degenerationshassan qureshiNo ratings yet
- Retina - 4Th SemiDocument14 pagesRetina - 4Th SemiBob BinNo ratings yet
- Objective - Subjective Eye Examination-Referral System and When To ReferDocument56 pagesObjective - Subjective Eye Examination-Referral System and When To ReferClara Sainuka100% (1)
- Workshop-Anamnesis & Pemeriksaan Oftalmologi Seminar IDIDocument57 pagesWorkshop-Anamnesis & Pemeriksaan Oftalmologi Seminar IDIMichael FlynnNo ratings yet
- Thyroid Eye Disease: - Varshaa BDocument16 pagesThyroid Eye Disease: - Varshaa BRia SharmaNo ratings yet
- Cornea: Anatomy & PhysiologyDocument68 pagesCornea: Anatomy & Physiologyadeline0% (1)
- Glaucoma and The Optic NerveDocument113 pagesGlaucoma and The Optic Nervepqwoeifjpakou134No ratings yet
- Diabetic Retinopathy: Dwi Lestari PohanDocument72 pagesDiabetic Retinopathy: Dwi Lestari PohanKelvin MandelaNo ratings yet
- CsfcsfasfafsaxchgfjjjDocument1 pageCsfcsfasfafsaxchgfjjjShabrina Ghassani RozaNo ratings yet
- Ketamine and Propdfofol in CircumsicionDocument4 pagesKetamine and Propdfofol in CircumsicionShabrina Ghassani RozaNo ratings yet
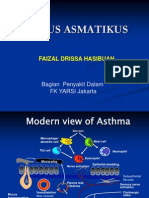
- Status Asmatikus FDH2012Document31 pagesStatus Asmatikus FDH2012Shabrina Ghassani Roza0% (1)
- Effect POF Kepada TubuhDocument5 pagesEffect POF Kepada TubuhShabrina Ghassani RozaNo ratings yet
- Antikonv Des 2012Document22 pagesAntikonv Des 2012Shabrina Ghassani RozaNo ratings yet
- Slide Head Injury ZickyDocument41 pagesSlide Head Injury ZickyShabrina Ghassani RozaNo ratings yet
- Asal Unduh AjaDocument1 pageAsal Unduh AjaShabrina Ghassani RozaNo ratings yet
- Periodic Test 2 Eco Class-12Document4 pagesPeriodic Test 2 Eco Class-12amandeep malikNo ratings yet
- Electromyography & It's Application in OrthodonticsDocument22 pagesElectromyography & It's Application in Orthodonticsprasadgayake100% (1)
- Midwives and Nutrition Education During Pregnancy - A Literature RDocument23 pagesMidwives and Nutrition Education During Pregnancy - A Literature RSuredaNo ratings yet
- TOPHEALTH SUNOF+ Ethylhexyl-P-Methoxycinnamate, 2-Ethylhexy MsdsDocument7 pagesTOPHEALTH SUNOF+ Ethylhexyl-P-Methoxycinnamate, 2-Ethylhexy MsdsTOP HEALTH ALRROMINo ratings yet
- Digestive SystemDocument27 pagesDigestive SystemLealyn Martin BaculoNo ratings yet
- P9 Lecture Child Abuse PDFDocument53 pagesP9 Lecture Child Abuse PDFVira PebrianaNo ratings yet
- CCC Breast Feeding PolicyDocument1 pageCCC Breast Feeding PolicyVictorNo ratings yet
- Funda Rle Reviewer - (Prelims)Document8 pagesFunda Rle Reviewer - (Prelims)Jhaztene Mae BaniquedNo ratings yet
- Senile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyDocument6 pagesSenile Cataract (Age-Related Cataract) : Practice Essentials, Background, PathophysiologyadliahghaisaniNo ratings yet
- INGREDIENTSDocument17 pagesINGREDIENTSPaulo BacayNo ratings yet
- Heart BNHADocument13 pagesHeart BNHAX OloGyNo ratings yet
- Heat StrokeDocument4 pagesHeat StrokeGerald YasonNo ratings yet
- Ulvac Ulvoil r7Document5 pagesUlvac Ulvoil r7Hiskia Benindo PurbaNo ratings yet
- BiomassDocument7 pagesBiomassJhonatan Romero HuarcayaNo ratings yet
- Your Electricity BillDocument8 pagesYour Electricity BillE EeNo ratings yet
- Sudeep SrivastavaDocument202 pagesSudeep Srivastavasandeepsrivastava41No ratings yet
- How The Red Cross Raised Half A Billion Dollars For Haiti - and Built Six Homes - ProPublicaDocument15 pagesHow The Red Cross Raised Half A Billion Dollars For Haiti - and Built Six Homes - ProPublicaGina PistolNo ratings yet
- Mental Practice in Chronic StrokeDocument6 pagesMental Practice in Chronic StrokeIsa AbdantauhidNo ratings yet
- DBE South African Sign Language National Catalogue 2018Document7 pagesDBE South African Sign Language National Catalogue 2018Anonymous ozd4aLKhNo ratings yet
- ADHD and The Endocannabinoid SystemDocument11 pagesADHD and The Endocannabinoid Systempn100% (1)
- Developmental Screening Tools: Michelle M. Macias, MD D-PIP Training Workshop June 16, 2006Document39 pagesDevelopmental Screening Tools: Michelle M. Macias, MD D-PIP Training Workshop June 16, 2006psy22No ratings yet
- Article in Press: Age-Related Hair Changes in Men: Mechanisms and Management of Alopecia and GrayingDocument5 pagesArticle in Press: Age-Related Hair Changes in Men: Mechanisms and Management of Alopecia and Grayingpasid harlisaNo ratings yet
- Letter To Seafarer Oct 26 2021Document2 pagesLetter To Seafarer Oct 26 2021Lynndon MagallanesNo ratings yet
- Diseases in Asian Aquaculture VIIDocument405 pagesDiseases in Asian Aquaculture VIIBurhan YusufNo ratings yet
- College Now Summer 2014 ApplicationDocument7 pagesCollege Now Summer 2014 ApplicationcollegeofficeNo ratings yet