You might also like
- Abortion and Sterilization: Medical and Social AspectsFrom EverandAbortion and Sterilization: Medical and Social AspectsJane E. HodgsonNo ratings yet
- Intrauterine Growth Restriction: Romy Mansour OBGYN Rotation October 2021Document52 pagesIntrauterine Growth Restriction: Romy Mansour OBGYN Rotation October 2021Romy MansourNo ratings yet
- Intrauterine Growth RestrictionDocument4 pagesIntrauterine Growth RestrictionFate ZephyrNo ratings yet
- Preterm Labour: Muhammad Hanif Final Year MBBSDocument32 pagesPreterm Labour: Muhammad Hanif Final Year MBBSArslan HassanNo ratings yet
- Bleeding in Early PregnancyDocument53 pagesBleeding in Early PregnancyTemahlungwaneNo ratings yet
- 1-Cardiac Disease With PregnancyDocument46 pages1-Cardiac Disease With PregnancyDrMohammad KhadrawyNo ratings yet
- Acute Abdomen During Pregnancy BelaynehDocument47 pagesAcute Abdomen During Pregnancy BelaynehYohannis AsefaNo ratings yet
- High Risk PregnancyDocument33 pagesHigh Risk PregnancyDakshayini MbNo ratings yet
- Breech Presentation 1Document16 pagesBreech Presentation 1api-3705046100% (1)
- Intrauterine Growth RestrictionDocument7 pagesIntrauterine Growth RestrictionNurfazlinaNo ratings yet
- Postterm PregnancyDocument16 pagesPostterm PregnancyrranindyaprabasaryNo ratings yet
- Neonatal MeningitisDocument10 pagesNeonatal MeningitisRana KhairunnisaNo ratings yet
- AUBDocument45 pagesAUBJBNo ratings yet
- Post Partum ComplicationDocument29 pagesPost Partum ComplicationPutri Rizky AmaliaNo ratings yet
- Care of The Pregnant Woman With HIVDocument34 pagesCare of The Pregnant Woman With HIVJenelle Melinda TullochNo ratings yet
- Preterm Labour: Pembimbing: Dr. Andriana Kumala Dewi, SP - OGDocument33 pagesPreterm Labour: Pembimbing: Dr. Andriana Kumala Dewi, SP - OGJovian LutfiNo ratings yet
- Gynecology Screening ProceduresDocument30 pagesGynecology Screening Proceduresapi-506496190No ratings yet
- Management of Hiv Positive Pregnant WomanDocument25 pagesManagement of Hiv Positive Pregnant Womanapi-3823785No ratings yet
- Dysfunctional Uterine BleedingDocument7 pagesDysfunctional Uterine BleedingNhorz Love UNo ratings yet
- Abnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadDocument35 pagesAbnormal Uterine Bleeding: - Rou'a Eyad - Rahaf EyadYazeed Asrawi0% (1)
- Demo KMC PDFDocument13 pagesDemo KMC PDFDiksha DuhanNo ratings yet
- Medical DisordersDocument225 pagesMedical DisordersWael GaberNo ratings yet
- Infertilityseminarppt 190718134710Document77 pagesInfertilityseminarppt 190718134710subiNo ratings yet
- Ovarian TorsionDocument48 pagesOvarian Torsionmaria ilyasNo ratings yet
- Prenatal TestingDocument26 pagesPrenatal TestingMar ClrNo ratings yet
- LBW, Care & FeedingDocument34 pagesLBW, Care & FeedingManju KumariNo ratings yet
- Abnormal Uterine Bleeding (AUB)Document45 pagesAbnormal Uterine Bleeding (AUB)asdf0% (1)
- Gestational Trophoblastic Disease GTDDocument39 pagesGestational Trophoblastic Disease GTDDea Maulidia100% (1)
- Fetal SkullDocument40 pagesFetal Skullsapana shah100% (1)
- PDFDocument8 pagesPDFSaumya SharmaNo ratings yet
- Theories of Labor OnsetDocument1 pageTheories of Labor OnsetWeng Maesa MontemayorNo ratings yet
- Uv Prolapse: Shehryar Shaikh Jarry Masood Fahim Rizvi Ashar MoinuddinDocument26 pagesUv Prolapse: Shehryar Shaikh Jarry Masood Fahim Rizvi Ashar MoinuddinSyeda Shariqa AnjumNo ratings yet
- APHDocument40 pagesAPHJayarani AshokNo ratings yet
- Intrauterine Insemination (IUI)Document6 pagesIntrauterine Insemination (IUI)AliaSyafiqaNo ratings yet
- Birth Injuries: Dr. Alsayed Alsharkawy Senior Pediatric Lecturer Widad University CollegeDocument35 pagesBirth Injuries: Dr. Alsayed Alsharkawy Senior Pediatric Lecturer Widad University CollegeEllis NabilaNo ratings yet
- Postpartum HemorrhageDocument20 pagesPostpartum Hemorrhagem_amroellahNo ratings yet
- Disorders During PregnancyDocument12 pagesDisorders During PregnancyazlanNo ratings yet
- Neonatal Respiratory DisordersDocument68 pagesNeonatal Respiratory Disorderslordoftheweb100% (25)
- ON Hemorrhage in Late Pregnancy, Placenta Previa and Abruptio PlacentaDocument22 pagesON Hemorrhage in Late Pregnancy, Placenta Previa and Abruptio PlacentaReshma AnilkumarNo ratings yet
- Prolonged LabourDocument3 pagesProlonged Labourgeorgeloto12No ratings yet
- Ultra Sound in PregnancyDocument77 pagesUltra Sound in Pregnancyhussain AltaherNo ratings yet
- Deep Vein Thrombosis in Pregnancy - Epidemiology, Pathogenesis, and Diagnosis - UpToDateDocument26 pagesDeep Vein Thrombosis in Pregnancy - Epidemiology, Pathogenesis, and Diagnosis - UpToDateCristinaCaprosNo ratings yet
- PuerperiumDocument16 pagesPuerperiumJSeashark100% (1)
- Ectopic Pregnancy (Autosaved)Document56 pagesEctopic Pregnancy (Autosaved)susmita shresthaNo ratings yet
- Hepatitis B in PregnancyDocument17 pagesHepatitis B in PregnancysnazzyNo ratings yet
- Infertility: Reshmi SibyDocument80 pagesInfertility: Reshmi SibySusan ThomasNo ratings yet
- Final PresentationDocument62 pagesFinal PresentationMacabio Zeil Love100% (1)
- Seminor Topic AbortionDocument13 pagesSeminor Topic AbortionBHUKYA USHARANINo ratings yet
- Birth Defects and Prenatal DiagnosisDocument137 pagesBirth Defects and Prenatal DiagnosisSohera Nadeem100% (1)
- Malformation of Female Reproductive SystemDocument170 pagesMalformation of Female Reproductive SystemKriti BanstolaNo ratings yet
- Neonatal Hematologic ConditionsDocument2 pagesNeonatal Hematologic ConditionsDelphy Varghese100% (1)
- Presented by DR - Shahbaz Ahmad Professor of Community MedicineDocument76 pagesPresented by DR - Shahbaz Ahmad Professor of Community MedicinePriya bhattiNo ratings yet
- Post Partum HemorhageDocument7 pagesPost Partum HemorhageLithiya JoseNo ratings yet
- InfertilityDocument14 pagesInfertilityDrChauhanNo ratings yet
- HEMOLYTIC DISEASE OF THE NEWBORN - Docx PrintDocument6 pagesHEMOLYTIC DISEASE OF THE NEWBORN - Docx PrintJudy HandlyNo ratings yet
- Vasa PraeviaDocument14 pagesVasa Praeviakhadzx100% (2)
- I So ImmunizationDocument21 pagesI So ImmunizationaaaNo ratings yet
- 04 - Postterm PregnancyDocument33 pages04 - Postterm PregnancyClinton Franda Markus SitanggangNo ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- Guideline Newborn Afrika SelatanDocument102 pagesGuideline Newborn Afrika SelatanM. KurnNo ratings yet
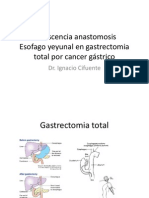
- Dehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástricoDocument22 pagesDehiscencia Anastomosis Esofago Yeyunal en Gastrectomia Total Por Cancer GástriconachooooooooNo ratings yet
- O&G LO SlidesDocument60 pagesO&G LO Slideskatherine nunnNo ratings yet
- Act G ManualDocument10 pagesAct G ManualMayjie CummosNo ratings yet
- FMStudent OME VideoGuideForFMDocument4 pagesFMStudent OME VideoGuideForFMR. H. SiddiquiNo ratings yet
- AFP Vision 2028: A World-Class Armed Forces, Source of National PrideDocument2 pagesAFP Vision 2028: A World-Class Armed Forces, Source of National PrideLevy Garcia SanchezNo ratings yet
- Specialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustDocument20 pagesSpecialty Doctor in ICU and Anaesthetics Job Description: East and North Hertfordshire NHS TrustjahangirealamNo ratings yet
- SEMINAR On - Doc High RiskDocument21 pagesSEMINAR On - Doc High RiskDivya Grace100% (3)
- The Neonatal Airway and Neonatal IntubationDocument32 pagesThe Neonatal Airway and Neonatal IntubationSubas SharmaNo ratings yet
- Factors Influencing The Role of Primary CareDocument10 pagesFactors Influencing The Role of Primary CareAdhiw AmanNo ratings yet
- Physiotherapy in Obstetrics and GynaecologyDocument493 pagesPhysiotherapy in Obstetrics and GynaecologyShanu Gal84% (19)
- TTNDocument10 pagesTTNsiti nur indahNo ratings yet
- Ectopic PregnancyDocument26 pagesEctopic PregnancysandhyakrishnanNo ratings yet
- Obs&GYN 1Document5 pagesObs&GYN 1AbedelrahmanShekhAhmadNo ratings yet
- Alabama Physicians LetterDocument12 pagesAlabama Physicians LetterJohn ArchibaldNo ratings yet
- Arnica The Miracle RemedyDocument10 pagesArnica The Miracle RemedyAnand GuptaNo ratings yet
- TOG 2023 Volume 25 Issue 3Document86 pagesTOG 2023 Volume 25 Issue 3saeed hasan saeedNo ratings yet
- Basic of Ophthalmology ExaminationsDocument47 pagesBasic of Ophthalmology ExaminationsAnonymous iy7I3o100% (2)
- Exp 4study of Local Anesthetics by Surface Anaesthesia On The Cornea of Rabbits - LabmonkDocument5 pagesExp 4study of Local Anesthetics by Surface Anaesthesia On The Cornea of Rabbits - LabmonkSubodh ShahNo ratings yet
- Anexa 1A IMM UltraDocument15 pagesAnexa 1A IMM UltraGabriela Diana MedlineNo ratings yet
- CsDocument7 pagesCsakosiMJcutie100% (1)
- Shunt Calculation, NICVDDocument31 pagesShunt Calculation, NICVDNavojit ChowdhuryNo ratings yet
- Chemistry - I: TEST(s) Normal UNIT(s)Document1 pageChemistry - I: TEST(s) Normal UNIT(s)Muhammad SuhaibNo ratings yet
- 00.00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpDocument5 pages00.00 Reference Care Plan Tonsillectomy and Adnoidectomy Post OpMarya KemmieNo ratings yet
- Intestin Gros Si AnorectalDocument282 pagesIntestin Gros Si AnorectalPatricia IoanaNo ratings yet
- The Human Sexual Response Cycle Is A FourDocument3 pagesThe Human Sexual Response Cycle Is A FourLeonard AyoraNo ratings yet
- LAPORAN KEGIATAN RESIDENSI HARI KE 2 Di RS SIRIRAJDocument24 pagesLAPORAN KEGIATAN RESIDENSI HARI KE 2 Di RS SIRIRAJIhrom Fatma SaputriNo ratings yet
- HBI Blacklist Journals 2018Document123 pagesHBI Blacklist Journals 2018pptpptNo ratings yet
- 484-Article Text-2583-1-10-20210630Document8 pages484-Article Text-2583-1-10-20210630Nova RizkenNo ratings yet
- Directorate General of Nursing & Midwifery Data Collection ToolDocument2 pagesDirectorate General of Nursing & Midwifery Data Collection ToolTama Roy89% (9)