You might also like
- Fast Facts: Pyruvatkinase-Mangel für Patienten und Angehörige: Eine seltene genetische Erkrankung der roten Blutkörperchen Informationen + Mitreden-Können = Bestmöglicher VerlaufFrom EverandFast Facts: Pyruvatkinase-Mangel für Patienten und Angehörige: Eine seltene genetische Erkrankung der roten Blutkörperchen Informationen + Mitreden-Können = Bestmöglicher VerlaufNo ratings yet
- Fast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoFrom EverandFast Facts: Deficiencia de piruvato quinasa para pacientes y familiares: Una enfermedad genética rara que afecta a los glóbulos rojos Información + Asumir el control = El mejor resultadoNo ratings yet
- Fluid Management and Shock ResuscitationDocument35 pagesFluid Management and Shock ResuscitationAsrarudin HamidNo ratings yet
- Fluid Student 2012Document43 pagesFluid Student 2012Sara Ilyas KhanNo ratings yet
- Fluids&Lytes PediatricDocument33 pagesFluids&Lytes Pediatricnugraha_esaNo ratings yet
- Fluid ManagementDocument10 pagesFluid ManagementdradaadNo ratings yet
- Fluids and Electrolytes in Pediatrics FinalDocument41 pagesFluids and Electrolytes in Pediatrics FinalArun GeorgeNo ratings yet
- Fluidsrenalacid BasebloodDocument8 pagesFluidsrenalacid BasebloodmyscribeNo ratings yet
- Fluid Management and Shock ResuscitationDocument32 pagesFluid Management and Shock ResuscitationKhoirul Tn Antik0% (1)
- Fluid and Electrolytes 1.Document26 pagesFluid and Electrolytes 1.Ethan LimNo ratings yet
- Urgentno Zbrinjavanje Dehidracije Kod Dece EngDocument43 pagesUrgentno Zbrinjavanje Dehidracije Kod Dece EngMirko BelanNo ratings yet
- Management of DKA PresentationDocument46 pagesManagement of DKA PresentationMuhammed YesufNo ratings yet
- Parenteral Fluid TherapyDocument5 pagesParenteral Fluid TherapyAbdalrahman KhalilNo ratings yet
- Fluid and Electrolytes: Robert Mcintyre, Jr. Associate Professor of Surgery University of Colorado Health Sciences CenterDocument54 pagesFluid and Electrolytes: Robert Mcintyre, Jr. Associate Professor of Surgery University of Colorado Health Sciences CenterWilliam Yap WLNo ratings yet
- Kenzu B, (MD, Asst - Professor of Surgery)Document40 pagesKenzu B, (MD, Asst - Professor of Surgery)kenzu bedruNo ratings yet
- Body Fluids and ElectrolytesDocument42 pagesBody Fluids and ElectrolytesQusaiBadr100% (1)
- Balance Cairan Final.Document41 pagesBalance Cairan Final.Niqko Bayu PrakarsaNo ratings yet
- Diarrhea and DehydrationDocument12 pagesDiarrhea and DehydrationnikprovNo ratings yet
- Fluid and Electrolyte TherapyDocument23 pagesFluid and Electrolyte TherapyJamal ArizonaNo ratings yet
- Rhabdomyolysis Case Study WeeblyDocument18 pagesRhabdomyolysis Case Study Weeblyapi-241865788No ratings yet
- Sagraves MSfluids Lytes 2004Document59 pagesSagraves MSfluids Lytes 2004Burhan Ul HaqNo ratings yet
- Fluid Management & Shock Resuscitation KGD SMT 7 PDFDocument34 pagesFluid Management & Shock Resuscitation KGD SMT 7 PDFTikuqNyukUnyukUnyuk100% (1)
- Fluid & Electrolite Management in Surgical WardsDocument97 pagesFluid & Electrolite Management in Surgical WardsBishwanath PrasadNo ratings yet
- PPC15 FEN SlidesDocument88 pagesPPC15 FEN SlidesbrianzflNo ratings yet
- Fluid and Blood TherapyDocument84 pagesFluid and Blood Therapyjean uwakijijweNo ratings yet
- Fluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversityDocument61 pagesFluid Management: Suparto Anesthesia Department Medical Faculty Christian Krida Wacana UniversitygozaNo ratings yet
- Fetus Term Infant Premature Infants 1 Year of Life Puberty: 1.) Intracellular Fluid (Icf)Document49 pagesFetus Term Infant Premature Infants 1 Year of Life Puberty: 1.) Intracellular Fluid (Icf)binsky2009No ratings yet
- Fluid & Electrolytes SaurabhDocument88 pagesFluid & Electrolytes Saurabhunknownsince1986No ratings yet
- Fluid Therapy Final 2019 DR TaanoDocument39 pagesFluid Therapy Final 2019 DR TaanoCabdi WaliNo ratings yet
- HONK by AijazDocument40 pagesHONK by AijazMuhammad Imran AlamNo ratings yet
- DehydrationDocument14 pagesDehydrationReimer LaquihuanacoNo ratings yet
- Fluid & Electrolytes Balance NewDocument21 pagesFluid & Electrolytes Balance NewPamela Ria Aguinaldo HensonNo ratings yet
- Hyper Nat Re MiaDocument27 pagesHyper Nat Re MiaPankaj Kumar SinghNo ratings yet
- Hypovolemic ShockDocument27 pagesHypovolemic Shock'govamaniacs' Insave IVNo ratings yet
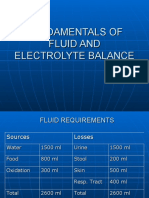
- Fundamentals of Fluid and Electrolyte BalanceDocument46 pagesFundamentals of Fluid and Electrolyte BalanceMelia Eka Rosita PharmacistNo ratings yet
- Intravenous Fluids: Composition & UsesDocument41 pagesIntravenous Fluids: Composition & UsesFathima BanuzNo ratings yet
- DkaDocument38 pagesDkaHam SotheaNo ratings yet
- Diabetic Ketoacidosis2Document2 pagesDiabetic Ketoacidosis2Venkat RamanNo ratings yet
- Internal Medicine TNDocument3 pagesInternal Medicine TNZeeshan Ahmed100% (2)
- Fluid - Electrolyte Imbalance 2012-InedDocument45 pagesFluid - Electrolyte Imbalance 2012-InedmiamuhpianNo ratings yet
- Disorders of Potassium Homeostasis: Informal Academic in ServiceDocument37 pagesDisorders of Potassium Homeostasis: Informal Academic in ServiceaqilasafikaNo ratings yet
- Pediatric NotesDocument45 pagesPediatric NoteskkkssbbNo ratings yet
- S.gaus-Management of Life-Threatening (Kuliah Sistem)Document54 pagesS.gaus-Management of Life-Threatening (Kuliah Sistem)Rusmin UsmanNo ratings yet
- Perioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud UniversityDocument47 pagesPerioperative Fluid Therapy: Department of Anesthesiology &ICU KKUH. King Saud Universityarifjo7999No ratings yet
- HyperkalemiaDocument30 pagesHyperkalemiaAyanna100% (3)
- Fluid Therapy and ElectroliteDocument36 pagesFluid Therapy and ElectroliteAriefBudimanHidayatNo ratings yet
- Fluid Resuscitation - Dita AditianingsihDocument48 pagesFluid Resuscitation - Dita AditianingsihGalih Wicaksono100% (1)
- Fluid & Electrolyte Balance: PresentedDocument30 pagesFluid & Electrolyte Balance: PresentedFathimathNo ratings yet
- Intravenous Fluid Therapy: Michael OrnesDocument27 pagesIntravenous Fluid Therapy: Michael OrnesOkto Mara Fandi HarahapNo ratings yet
- Fluid & Electrolyte TherapyDocument38 pagesFluid & Electrolyte Therapyharjuna100% (1)
- Kelly Shinkaruk, MD FRCPC HLT 123 October 17, 2009Document88 pagesKelly Shinkaruk, MD FRCPC HLT 123 October 17, 2009Hutagaol ImeldaNo ratings yet
- 120 Med Labs HyperkalaemiaDocument4 pages120 Med Labs HyperkalaemiaqurbanNo ratings yet
- Fluids & Electrolytes Acid/Bas Balance: DR Wael SadaqahDocument72 pagesFluids & Electrolytes Acid/Bas Balance: DR Wael Sadaqahdr wael sadaqaNo ratings yet
- Surgery 1.1 Fluid and Electrolyte Balance - Azares PDFDocument7 pagesSurgery 1.1 Fluid and Electrolyte Balance - Azares PDFAceking MarquezNo ratings yet
- Roumilla Mendoza, M.D. Roumilla Mendoza, M.D. Pediatric Gastroenterologist Pediatric GastroenterologistDocument59 pagesRoumilla Mendoza, M.D. Roumilla Mendoza, M.D. Pediatric Gastroenterologist Pediatric GastroenterologistYenyen DelgadoNo ratings yet
- Somchodok Chakreeyarat, MD. Endocrine Unit, Department of Medicine Bhumibol Adulyadej HospitalDocument53 pagesSomchodok Chakreeyarat, MD. Endocrine Unit, Department of Medicine Bhumibol Adulyadej HospitalLing TaerahkunNo ratings yet
- Terapi Cairan Dan Transfusi: Dr. Imam Ghozali., Span.,MkesDocument47 pagesTerapi Cairan Dan Transfusi: Dr. Imam Ghozali., Span.,MkesHelend ChildDjNo ratings yet
- UMBC CC-EMTP Class Notes, FLCC Class 2010Document93 pagesUMBC CC-EMTP Class Notes, FLCC Class 2010Marc LaBarberaNo ratings yet
- Potassium Final2Document18 pagesPotassium Final2Kholoud KholoudNo ratings yet
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansFrom EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpNo ratings yet
- ShockDocument21 pagesShockIgor StefanetNo ratings yet
- ShockDocument36 pagesShockMin-Joo Esther ParkNo ratings yet
- Shock and HypoperfusionDocument46 pagesShock and HypoperfusionIgor StefanetNo ratings yet
- ShockDocument28 pagesShockIgor StefanetNo ratings yet
- Shock I and IIDocument105 pagesShock I and IIIgor StefanetNo ratings yet
- Shock 4813Document18 pagesShock 4813docprashNo ratings yet
- Shock: Differential Diagnosis and Hemodynamic MonitoringDocument21 pagesShock: Differential Diagnosis and Hemodynamic MonitoringtataranyNo ratings yet
- Septic ShockDocument50 pagesSeptic ShockIgor StefanetNo ratings yet
- Lesson 5Document14 pagesLesson 5Igor StefanetNo ratings yet
- EMS Shock LexDocument60 pagesEMS Shock LexIgor StefanetNo ratings yet
- Ramphal SepsisDocument29 pagesRamphal SepsisIgor StefanetNo ratings yet
- Pharmacotherapy of ShockDocument23 pagesPharmacotherapy of ShockIgor Stefanet100% (2)
- Cardiogenic Shock - FINALDocument79 pagesCardiogenic Shock - FINALIgor StefanetNo ratings yet
- Cardiogenic ShockDocument27 pagesCardiogenic ShockIgor StefanetNo ratings yet
- 2008 Corrective Hair Transplant ArticleDocument9 pages2008 Corrective Hair Transplant ArticleIgor StefanetNo ratings yet
- Blood TherapyDocument21 pagesBlood TherapySandra Ag Ariodere KeonyediNo ratings yet
- Treatment of Venous Thrombosis and Pulmonary EmbolismDocument53 pagesTreatment of Venous Thrombosis and Pulmonary EmbolismIgor StefanetNo ratings yet
- Transplant Balding ScalpDocument8 pagesTransplant Balding ScalpIgor StefanetNo ratings yet
- 5 Big Tournament LeaksDocument17 pages5 Big Tournament LeaksIgor StefanetNo ratings yet
- Toshiba Conditioner PDFDocument73 pagesToshiba Conditioner PDFIgor StefanetNo ratings yet
- GERIAT1Document8 pagesGERIAT1Igor StefanetNo ratings yet
- 10 More Essential HoldDocument51 pages10 More Essential HoldIgor StefanetNo ratings yet
- BinionDocument75 pagesBinionIgor StefanetNo ratings yet
- Digestion Enzyme Practice TestDocument15 pagesDigestion Enzyme Practice TestJila HafiziNo ratings yet
- Anterior Cross Bites in Primary Mixed Dentition PedoDocument32 pagesAnterior Cross Bites in Primary Mixed Dentition PedoFourthMolar.comNo ratings yet
- 21 Prof Suwadi DEVIASI SEXDocument46 pages21 Prof Suwadi DEVIASI SEXdr.cintaNo ratings yet
- SIL (2011) List of Semantic DomainsDocument19 pagesSIL (2011) List of Semantic DomainsTakashi NakagawaNo ratings yet
- Atlas of Poultry Disease 2Document41 pagesAtlas of Poultry Disease 2DDurasNo ratings yet
- TugasDocument4 pagesTugasYuli Wardani OrNo ratings yet
- Editorial For December 2010 - Rare RemediesDocument4 pagesEditorial For December 2010 - Rare Remediespanniyin selvanNo ratings yet
- Pentavet Homeopathic Veterinary Medicine For AnorexiaDocument16 pagesPentavet Homeopathic Veterinary Medicine For AnorexiaLonely WolfNo ratings yet
- 7 Habits Checklist1 1 PDFDocument3 pages7 Habits Checklist1 1 PDFilsarduNo ratings yet
- Fish Poisoning (Print)Document65 pagesFish Poisoning (Print)Cristina SarinoNo ratings yet
- DLLDocument7 pagesDLLmichelle abianNo ratings yet
- Subcutaneous MycosesDocument22 pagesSubcutaneous MycosesIan MosesNo ratings yet
- Basic Cardiac Life Support 2011Document6 pagesBasic Cardiac Life Support 2011Tashfeen Bin NazeerNo ratings yet
- J 1365-2869 2012 01044 XDocument371 pagesJ 1365-2869 2012 01044 XMarco Bakker100% (1)
- Chapter 2 Body CoordinationDocument15 pagesChapter 2 Body CoordinationYatt YatiNo ratings yet
- Honk ScriptDocument48 pagesHonk ScriptTom Corcoran100% (4)
- Malaria Control BrochureDocument2 pagesMalaria Control BrochureEkwoh Okwuchukwu ENo ratings yet
- Being Afraid: Everyday WorriesDocument10 pagesBeing Afraid: Everyday Worriesdina171279No ratings yet
- 2 Medrega Cristian Gabriel enDocument1 page2 Medrega Cristian Gabriel enCristian GabrielNo ratings yet
- Anatomi Dan Fisiologi GinjalDocument32 pagesAnatomi Dan Fisiologi GinjalAlamul Huda100% (1)
- Vitamin B ComplexDocument3 pagesVitamin B Complexjoseph_delacruz20No ratings yet
- Middle Cerebral Artery DopplerDocument4 pagesMiddle Cerebral Artery DopplerHervi LaksariNo ratings yet
- PPK ParuDocument64 pagesPPK Parusri wahyuniNo ratings yet
- Health AssessmentDocument39 pagesHealth AssessmentAnnalisa TellesNo ratings yet
- Aquarium Pharmaceuticals AmmoniaDocument1 pageAquarium Pharmaceuticals AmmoniaKayyyNo ratings yet
- Sjavs 24a270 281Document12 pagesSjavs 24a270 281Ramesh BeniwalNo ratings yet
- Indian Meat Industry: Opportunities and Challenges: January 2011Document7 pagesIndian Meat Industry: Opportunities and Challenges: January 2011satyajitNo ratings yet
- TURP SyndromeDocument13 pagesTURP SyndromeWindy Ari WijayaNo ratings yet
- Topic Test: Oxfordaqa International Gcse Biology 9201Document26 pagesTopic Test: Oxfordaqa International Gcse Biology 9201Novanolo Christovori ZebuaNo ratings yet
- Horner SYndromeDocument3 pagesHorner SYndromeHendri Wijaya WangNo ratings yet