You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Scared SickDocument320 pagesScared SickChapali100% (5)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- NSO Class 8 Solved Sample PaperDocument8 pagesNSO Class 8 Solved Sample Papergopi_dey8649100% (1)
- Lourdes College Nursing Program Drug StudyDocument2 pagesLourdes College Nursing Program Drug Studypinksapphire929100% (2)
- Pathophysiology of Diabetes Mellitus Type 2Document7 pagesPathophysiology of Diabetes Mellitus Type 2jnrue_aerith96% (28)
- PSUR Instructions - FinalDocument20 pagesPSUR Instructions - Finalgopi_dey8649No ratings yet
- Defibrillator: DR Sumanth ReddyDocument39 pagesDefibrillator: DR Sumanth Reddyrohith100% (1)
- Lyme Disease and Tick-Born Co-Infections: Emily Maiella N.D. Montague Integrative Health 413.230.4462Document79 pagesLyme Disease and Tick-Born Co-Infections: Emily Maiella N.D. Montague Integrative Health 413.230.4462Manasi PalavNo ratings yet
- Bilirubin Metabolism: Hd. - Msc. (Biochemistry)Document18 pagesBilirubin Metabolism: Hd. - Msc. (Biochemistry)MuhamadMarufNo ratings yet
- Lee Meningiomas PDFDocument615 pagesLee Meningiomas PDFVineesh VargheseNo ratings yet
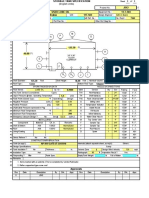
- API 650 Tank Design 1Document5 pagesAPI 650 Tank Design 1robertantoreni100% (9)
- Turbine Operation Manual 600 MW DongfangDocument223 pagesTurbine Operation Manual 600 MW Dongfangkumar_ranjan_373% (11)
- Curves in SpaceDocument7 pagesCurves in Spacegopi_dey8649No ratings yet
- Up Ps CadverDocument11 pagesUp Ps CadverJeshiNo ratings yet
- Ones Assignment Method for Solving Traveling Salesman ProblemDocument8 pagesOnes Assignment Method for Solving Traveling Salesman Problemgopi_dey8649No ratings yet
- Insightofindia Quiz 2016-0-123Document35 pagesInsightofindia Quiz 2016-0-123gopi_dey8649No ratings yet
- Vector Analysis Paper I Segment Wise Questions From 1983 To 2011Document6 pagesVector Analysis Paper I Segment Wise Questions From 1983 To 2011gopi_dey8649No ratings yet
- Preclinical Research Clinical Research Nda Review Phase I NDA Basic Science ResearchDocument1 pagePreclinical Research Clinical Research Nda Review Phase I NDA Basic Science Researchgopi_dey8649No ratings yet
- Iec 4Document21 pagesIec 4gopi_dey8649No ratings yet
- UPSC IAS Mains Exam Paper 2014 General Studies Paper 1Document6 pagesUPSC IAS Mains Exam Paper 2014 General Studies Paper 1Santosh AvhadNo ratings yet
- Maths Book List - BipinDocument1 pageMaths Book List - Bipingopi_dey8649No ratings yet
- IAS Mains Exam Paper 2014 General Studies Paper 2Document10 pagesIAS Mains Exam Paper 2014 General Studies Paper 2gopi_dey8649No ratings yet
- General Studies Economics Part IDocument22 pagesGeneral Studies Economics Part IbusisubbareddyNo ratings yet
- Cbse - Biz: Paper Prepared byDocument3 pagesCbse - Biz: Paper Prepared bygopi_dey8649No ratings yet
- Kesavandana Bharti CaseDocument3 pagesKesavandana Bharti Casegopi_dey8649No ratings yet
- KksDocument78 pagesKksgopi_dey8649No ratings yet
- Visionias PubadDocument6 pagesVisionias Pubadgopi_dey8649No ratings yet
- Jadavpur BrocureDocument16 pagesJadavpur Brocuregopi_dey8649No ratings yet
- Electricity UntDocument1 pageElectricity Untgopi_dey8649No ratings yet
- Kesavandana Bharti CaseDocument3 pagesKesavandana Bharti Casegopi_dey8649No ratings yet
- System Head CurveDocument1 pageSystem Head Curvegopi_dey8649No ratings yet
- p13036 Lanco 55 MW Ed-1 A121218 Performance PDFDocument3 pagesp13036 Lanco 55 MW Ed-1 A121218 Performance PDFgopi_dey8649No ratings yet
- ClarificationSolar PV - Thermal PDFDocument18 pagesClarificationSolar PV - Thermal PDFgopi_dey8649No ratings yet
- System Head CurveDocument1 pageSystem Head Curvegopi_dey8649No ratings yet
- I2-08-00249-01.3.1 Ed3 c070427 PerformanceDocument6 pagesI2-08-00249-01.3.1 Ed3 c070427 Performancegopi_dey8649No ratings yet
- 01 Cover NoteDocument1 page01 Cover Notegopi_dey8649No ratings yet
- Thailand TripDocument6 pagesThailand Tripgopi_dey8649No ratings yet
- Classic Laryngeal Mask Airway Insertion With Laryngoscope Mcgrath and Macintosh: A Case SeriesDocument3 pagesClassic Laryngeal Mask Airway Insertion With Laryngoscope Mcgrath and Macintosh: A Case SeriesYeyen AgustinNo ratings yet
- 2019 - 2020 - Boston Immunization - Hult Immunization FormDocument4 pages2019 - 2020 - Boston Immunization - Hult Immunization FormOscar RomainvilleNo ratings yet
- Theme 2 - Partial Acrylic Removable Denture: Maxilla LimitsDocument3 pagesTheme 2 - Partial Acrylic Removable Denture: Maxilla LimitsShany SchwarzwaldNo ratings yet
- Different Types of Medicines ExplainedDocument3 pagesDifferent Types of Medicines ExplainedAngelique BernardinoNo ratings yet
- Diagnosis and Treatment of Forefoot Disorders. Section 4. Tailor's BunionDocument7 pagesDiagnosis and Treatment of Forefoot Disorders. Section 4. Tailor's BunionbaoNo ratings yet
- Turkey Position PaperDocument3 pagesTurkey Position PaperBill GatesNo ratings yet
- (Pediaii) - 021 - Disorders of The Respiratory TractDocument17 pages(Pediaii) - 021 - Disorders of The Respiratory TractdoktoraronaNo ratings yet
- BCBT-52822 - Lecture - Dulith AbeykoonDocument84 pagesBCBT-52822 - Lecture - Dulith Abeykoonkaneeshka namasivayamNo ratings yet
- Preventative Care Assignment-Part 24 AnswersDocument9 pagesPreventative Care Assignment-Part 24 AnswersOdia OaikhenaNo ratings yet
- Social Treatment in PsychiatryDocument17 pagesSocial Treatment in PsychiatryLawal Sikirat OpeyemiNo ratings yet
- Firs World Report PDFDocument35 pagesFirs World Report PDFMarv MarvNo ratings yet
- Infectious Bronchitis and Its Effect On Egg Production and Egg QualityDocument2 pagesInfectious Bronchitis and Its Effect On Egg Production and Egg QualityPrima Puji RaharjoNo ratings yet
- Post-Cesarean Recovery Progress NotesDocument2 pagesPost-Cesarean Recovery Progress NotesJam JamaNo ratings yet
- Arthrex ACP® Double SyringeDocument8 pagesArthrex ACP® Double SyringeMofit penjačka stijenaNo ratings yet
- 2 Pathophysiology EpidemiologyDocument36 pages2 Pathophysiology EpidemiologyYosefina CindyNo ratings yet
- Nursing Care Framework - Version 1Document22 pagesNursing Care Framework - Version 1chelissa maitaNo ratings yet
- Resume Nicole Chan 2Document3 pagesResume Nicole Chan 2api-291342331No ratings yet
- Heart SurgeonDocument8 pagesHeart SurgeonayaanmalikyaseenNo ratings yet
- Mifepristone & MisoprostolDocument6 pagesMifepristone & MisoprostolnanimadallaNo ratings yet
- ARTERISCLEROSISDocument46 pagesARTERISCLEROSISAdilla Edi AriefNo ratings yet
- Diseases of The Cornea Prof. Zoltán Zsolt NagyDocument123 pagesDiseases of The Cornea Prof. Zoltán Zsolt NagydebbyNo ratings yet
- NSW Faculty TRIAL FELLOWSHIP EXAMINATION Short Answer QuestionsDocument42 pagesNSW Faculty TRIAL FELLOWSHIP EXAMINATION Short Answer Questionssacabona50% (2)
- Aki VS CKDDocument2 pagesAki VS CKDKevin TranNo ratings yet