You might also like
- Chest Tube and Water-Seal DrainageDocument25 pagesChest Tube and Water-Seal DrainageGhadaNo ratings yet
- Nasopharyngeal Carcinoma: From Etiology to Clinical PracticeFrom EverandNasopharyngeal Carcinoma: From Etiology to Clinical PracticeAnne W.M. LeeNo ratings yet
- Lung BiopsyDocument8 pagesLung BiopsySiya PatilNo ratings yet
- Lung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesFrom EverandLung Metabolism: Proteolysis and Antioproteolysis Biochemical Pharmacology Handling of Bioactive SubstancesAlain JunodNo ratings yet
- Management of Lung CancerDocument31 pagesManagement of Lung CancerPadmaj KulkarniNo ratings yet
- Essential Concepts for Airway ManagementDocument42 pagesEssential Concepts for Airway Managementkader abdiNo ratings yet
- Empyema Thoracis: Ain Najwa BT Abd Rahim (090100457) MARDHIAH BT MARZUKI (090100470)Document22 pagesEmpyema Thoracis: Ain Najwa BT Abd Rahim (090100457) MARDHIAH BT MARZUKI (090100470)Dumora FatmaNo ratings yet
- Pneumonectomy S RT RpaDocument4 pagesPneumonectomy S RT RpagireeshsachinNo ratings yet
- Chest DrainsDocument22 pagesChest DrainsNuru99100% (3)
- Mediastinal Masses Imaging and LocalizationDocument110 pagesMediastinal Masses Imaging and Localizationosep77100% (1)
- Lung AuscultationDocument62 pagesLung AuscultationOlea CroitorNo ratings yet
- Chest Trauma FinalDocument50 pagesChest Trauma FinalAsim Siddiq VineNo ratings yet
- Acute Respiratory Distress SyndromeDocument30 pagesAcute Respiratory Distress SyndromeNikhil GhubadeNo ratings yet
- CHEst TraumaDocument20 pagesCHEst TraumajeorjNo ratings yet
- Modes of Mechanical VentilationDocument4 pagesModes of Mechanical Ventilationsgod34100% (1)
- Pediatric Lung Diseases: Empyema and Lung AbscessDocument39 pagesPediatric Lung Diseases: Empyema and Lung AbscessFaisal MoidunnyNo ratings yet
- Pulmonary SequestrationDocument15 pagesPulmonary SequestrationEmily EresumaNo ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- Flail Chest ReportDocument4 pagesFlail Chest ReportMiggsNo ratings yet
- Bronchial AsthmaDocument25 pagesBronchial AsthmaKamil HannaNo ratings yet
- Lung Cancer: By: Faezah Nur Mohd Redzwan Nooratiqah RahmatDocument30 pagesLung Cancer: By: Faezah Nur Mohd Redzwan Nooratiqah RahmatDumora FatmaNo ratings yet
- Initial Assessment and Management of Trauma PatientsDocument8 pagesInitial Assessment and Management of Trauma PatientsAlvin De LunaNo ratings yet
- Flail ChestDocument26 pagesFlail ChestStawan ChouguleNo ratings yet
- Ventricular Septal DefectsDocument7 pagesVentricular Septal DefectsMuhammadAldoGiansyahNo ratings yet
- Thoracoabdominal Aneurysm Surgery and The Risk of ParaplegiaDocument34 pagesThoracoabdominal Aneurysm Surgery and The Risk of ParaplegiaKhaled S. HarbNo ratings yet
- Advances in Emergent Airway Management in PediatricsDocument19 pagesAdvances in Emergent Airway Management in PediatricsLuis Miguel VillanuevaNo ratings yet
- The Management of Acute Respiratory Distress SyndromeDocument48 pagesThe Management of Acute Respiratory Distress SyndromeLauraAlvarezMulettNo ratings yet
- AtelectasisDocument43 pagesAtelectasismulan557100% (1)
- Student Refresher CourseDocument87 pagesStudent Refresher CourseRaisa S. MariscalNo ratings yet
- Difficult AirwayDocument77 pagesDifficult AirwayParvathy R Nair100% (1)
- Pneumonectomy 2Document7 pagesPneumonectomy 2jeanelineNo ratings yet
- Mic Cabg Procedure PDFDocument12 pagesMic Cabg Procedure PDFprofarmah6150No ratings yet
- FinalDocument56 pagesFinalvamshidhNo ratings yet
- Infective Endocarditis: An UpdateDocument66 pagesInfective Endocarditis: An UpdateDias SeptariiaNo ratings yet
- Current and Future Development in Lung Cancer Diagnosis: Molecular SciencesDocument18 pagesCurrent and Future Development in Lung Cancer Diagnosis: Molecular SciencesHeru SigitNo ratings yet
- DVT ProphylaxisDocument30 pagesDVT ProphylaxissivaNo ratings yet
- Intercostal DrainageDocument39 pagesIntercostal DrainagePutri AdiratnaNo ratings yet
- Lung Sounds: An Assessment of The Patient in Respiratory DistressDocument40 pagesLung Sounds: An Assessment of The Patient in Respiratory DistressJoseph Rodney de LeonNo ratings yet
- Mechanical Ventilation and Intracranial PressureDocument30 pagesMechanical Ventilation and Intracranial PressureFlavius AnghelNo ratings yet
- Thoracic Trauma: Kenyatta University LectureDocument25 pagesThoracic Trauma: Kenyatta University LectureIrene Zae MwandotoNo ratings yet
- Overview of Mechanical Ventilation Settings, Modes, TroubleshootingDocument24 pagesOverview of Mechanical Ventilation Settings, Modes, TroubleshootingRochim CoolNo ratings yet
- Centrel Venous CatheterizationDocument77 pagesCentrel Venous CatheterizationAli100% (1)
- CABG Case Study ReportDocument83 pagesCABG Case Study ReportSherena NicolasNo ratings yet
- Acute Pulmonary EmbolismDocument55 pagesAcute Pulmonary EmbolismEzzat Abdelhafeez Salem100% (1)
- Report EmpyemaDocument32 pagesReport EmpyemaMylah CruzNo ratings yet
- Suctioning Artificial Airways - AdultsDocument27 pagesSuctioning Artificial Airways - AdultssdaNo ratings yet
- Thoracic Decortication: Sabita Chalise Bns 3 YearDocument32 pagesThoracic Decortication: Sabita Chalise Bns 3 YearRamchandra Chalise100% (1)
- LungDocument427 pagesLungGeo GrigoreNo ratings yet
- Immediate Complications Following Thoracic SurgeryDocument17 pagesImmediate Complications Following Thoracic SurgeryPopa TiberiuNo ratings yet
- Principles of Laparoscopic & Robotic Surgery: Aaquila Sherin Bismi J J Blessy OommanDocument46 pagesPrinciples of Laparoscopic & Robotic Surgery: Aaquila Sherin Bismi J J Blessy OommanAsif AbbasNo ratings yet
- Epid COPDDocument9 pagesEpid COPDAgung WistaraNo ratings yet
- Baska MaskDocument8 pagesBaska MaskAnish H DaveNo ratings yet
- Endotracheal IntubationDocument33 pagesEndotracheal IntubationReza Dyan Perdani ZeinNo ratings yet
- Tetralogy of FallotDocument24 pagesTetralogy of FallotjustinahorroNo ratings yet
- OxygenationDocument50 pagesOxygenationLulu MushiNo ratings yet
- Thorax and The LungsDocument30 pagesThorax and The Lungschifunndo charles100% (1)
- Cardiopulmonary Bypass Machine - CPBDocument12 pagesCardiopulmonary Bypass Machine - CPBhadeel fahimNo ratings yet
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- Left-Sided Congestive Heart Failure Case PresentationDocument64 pagesLeft-Sided Congestive Heart Failure Case PresentationNicole Villanueva, BSN - Level 3ANo ratings yet
- Pectus Excavatum, Advanced Nuss ProcedureDocument34 pagesPectus Excavatum, Advanced Nuss ProcedurelmdarlongNo ratings yet
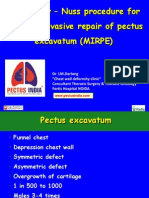
- Minimally Invasive Pectus Excavatum Repair TechniqueDocument7 pagesMinimally Invasive Pectus Excavatum Repair TechniquelmdarlongNo ratings yet
- Vats Bullectomy: Initial Shillong ExperienceDocument21 pagesVats Bullectomy: Initial Shillong ExperiencelmdarlongNo ratings yet
- Video Assisted Thoracic Surgery API TripuraDocument11 pagesVideo Assisted Thoracic Surgery API TripuralmdarlongNo ratings yet
- Pneumothorax: DR L.M.Darlong Ms (Aiims) Fellow Thoracic Surg (Seoul)Document13 pagesPneumothorax: DR L.M.Darlong Ms (Aiims) Fellow Thoracic Surg (Seoul)lmdarlong0% (1)
- CASE STUDY (Gastro)Document3 pagesCASE STUDY (Gastro)Jake Yvan DizonNo ratings yet
- Ivermectin For CancerDocument15 pagesIvermectin For CancerSheena FriesenNo ratings yet
- Pathology Lab.: Gastrointestinal Tract MD IvDocument27 pagesPathology Lab.: Gastrointestinal Tract MD IvPablo SisirucaNo ratings yet
- In Defense of Smokers by Lauren A ColbyDocument54 pagesIn Defense of Smokers by Lauren A ColbyScottyDog101100% (1)
- Management of Patients With Oral and Esophageal DisordersDocument14 pagesManagement of Patients With Oral and Esophageal Disordersintotheunknown100% (2)
- 10 Anos Cross Trial Jco2021Document11 pages10 Anos Cross Trial Jco2021alomeletyNo ratings yet
- Surgicl Pathology of OesophagusDocument91 pagesSurgicl Pathology of Oesophagusmikaaa000No ratings yet
- 2017 - Alcohol, Smoking and Risk of Esophago-Gastric CancerDocument9 pages2017 - Alcohol, Smoking and Risk of Esophago-Gastric CancerPatricia Peñaflor GrimaldoNo ratings yet
- Pathophysiology of Gastric CancerDocument2 pagesPathophysiology of Gastric CancerAjon Veloso100% (3)
- Medical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersDocument34 pagesMedical Surgical Nursing Module 1 Lesson 1 Upper Gastrointestinal DisordersRomelyn Ordillas100% (2)
- DIGESTIVE DISORDERSDocument10 pagesDIGESTIVE DISORDERSLeila Acero Salinas100% (1)
- Surgical Approaches To Esophageal CancerDocument6 pagesSurgical Approaches To Esophageal CancerYacine Tarik AizelNo ratings yet
- GI Internal Medicine PDFDocument9 pagesGI Internal Medicine PDFArianneJulienaCervaniaAndradaNo ratings yet
- The Human Microbiota in Health and Disease PDFDocument12 pagesThe Human Microbiota in Health and Disease PDFMariaNo ratings yet
- GIT DisordersDocument171 pagesGIT DisordersKatrina PonceNo ratings yet
- Upper GI Drugs (Pod Pharm 2023, Thatcher)Document39 pagesUpper GI Drugs (Pod Pharm 2023, Thatcher)8jm6dhjdcpNo ratings yet
- Chest Surgery DelhiDocument3 pagesChest Surgery DelhiAnonymous OrzzzvmnnDNo ratings yet
- Gastric Surgery MCQDocument6 pagesGastric Surgery MCQSajag GuptaNo ratings yet
- Dematos 1997Document6 pagesDematos 1997Ali AmokraneNo ratings yet
- A 1753 9801Document9 pagesA 1753 9801Mohammad ShaikhaniNo ratings yet
- نم انوسنت لا مكوجرأ ,يلهلا و يل ةيراج ةقدص مكئاعد حلا ص Please Grace us with your good prayersDocument538 pagesنم انوسنت لا مكوجرأ ,يلهلا و يل ةيراج ةقدص مكئاعد حلا ص Please Grace us with your good prayersSahan EpitawalaNo ratings yet
- Textbook of Gastrointestinal Oncology 2019Document711 pagesTextbook of Gastrointestinal Oncology 2019Juan Carlos Marcos Enriquez100% (1)
- Diagnosis and Treatment of Gastrointestinal CancersDocument230 pagesDiagnosis and Treatment of Gastrointestinal CancersSoyPedroNo ratings yet
- Gastroenterology: Maintenance of Certification (MOC) Examination BlueprintDocument11 pagesGastroenterology: Maintenance of Certification (MOC) Examination BlueprintAdson AlcantaraNo ratings yet
- Surgery Songbook CompressedDocument69 pagesSurgery Songbook CompressedBrandon HayashiNo ratings yet
- Caustic Injury of The Esophagus PDFDocument3 pagesCaustic Injury of The Esophagus PDFSpecialNameNo ratings yet
- Esophageal CancerDocument3 pagesEsophageal CancerChanthorn SokNo ratings yet
- 8th Edition AJCC/UICC Staging of Cancers of The Esophagus and Esophagogastric Junction: Application To Clinical PracticeDocument12 pages8th Edition AJCC/UICC Staging of Cancers of The Esophagus and Esophagogastric Junction: Application To Clinical PracticeGustavo UriondoNo ratings yet
- Comparison of Endoscopic Vacuum Therapy Versus Stent For Anastomotic Leak After EsophagectomyDocument7 pagesComparison of Endoscopic Vacuum Therapy Versus Stent For Anastomotic Leak After EsophagectomySergio Sitta TarquiniNo ratings yet
- NCI Validates Homoeopathic Cancer TreatmentDocument6 pagesNCI Validates Homoeopathic Cancer TreatmentSuraj YadavNo ratings yet