You might also like
- Example PPLB 76 Log BookDocument1 pageExample PPLB 76 Log BooklonstaNo ratings yet
- Case Study Spinal Cord Injury2Document3 pagesCase Study Spinal Cord Injury2kayevhin0533% (3)
- On Being Sane in Insane Places PDFDocument8 pagesOn Being Sane in Insane Places PDFEdirfNo ratings yet
- Pa Tho Physiology of Spinal Cord InjuryDocument1 pagePa Tho Physiology of Spinal Cord InjuryGenel Joseph Jacildo Peñaflor100% (2)
- Bacls PDFDocument23 pagesBacls PDFAngelo Domingo0% (1)
- Spinal Cord InjuryDocument28 pagesSpinal Cord InjurydidiNo ratings yet
- Patho Physiology Spinal Cord InjuryDocument2 pagesPatho Physiology Spinal Cord InjuryIris Caberte100% (1)
- Clinical Daily ChecklistDocument2 pagesClinical Daily ChecklistJane ChabaneNo ratings yet
- Clinical ExemplarDocument3 pagesClinical Exemplarapi-302122563No ratings yet
- PacemakerDocument63 pagesPacemakerMonish RautNo ratings yet
- Hair LaserDocument10 pagesHair Laseriship pkmkenangaNo ratings yet
- Spinal Cord InjuryDocument47 pagesSpinal Cord InjuryShitaljit IromNo ratings yet
- Spinal Cord InjuryDocument50 pagesSpinal Cord InjuryVINCHRISTINENo ratings yet
- Spinal Cord InjuryDocument33 pagesSpinal Cord InjuryNi Made Dwiki Andriyani100% (2)
- Spinal Cord InjuryDocument16 pagesSpinal Cord Injuryjohnlester_jlf100% (2)
- Spinal Cord Injury: Barrios, Kevin George BDocument52 pagesSpinal Cord Injury: Barrios, Kevin George B乔治凯文No ratings yet
- CvaDocument42 pagesCvad_94No ratings yet
- A Case Study ON Cerebrovascular Accident With Left HemiparesisDocument57 pagesA Case Study ON Cerebrovascular Accident With Left Hemiparesisdonheyzz_020% (1)
- Spinal Cord Injury: Causation & PathophysiologyDocument10 pagesSpinal Cord Injury: Causation & Pathophysiologycpradheep100% (3)
- Osteoarthritis 1583-170210113823Document34 pagesOsteoarthritis 1583-170210113823Angelic khanNo ratings yet
- Pathophysiology HeadinjuryDocument1 pagePathophysiology HeadinjuryK.b. Dequiña100% (1)
- Paget's Disease of The BoneDocument9 pagesPaget's Disease of The BonePam RomeroNo ratings yet
- Traumatic Brain InjuryDocument14 pagesTraumatic Brain InjurySamuel Hananiel RoryNo ratings yet
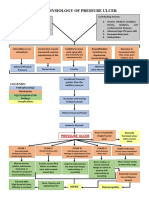
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- NCP CSDocument4 pagesNCP CSJM UncianoNo ratings yet
- Concept Map AAADocument6 pagesConcept Map AAASandrine BarredoNo ratings yet
- Myocardial InfractionDocument16 pagesMyocardial InfractionYAMINIPRIYANNo ratings yet
- Brief Description: Pleural EffusionDocument3 pagesBrief Description: Pleural EffusionJessica CatacutanNo ratings yet
- A Case Study On Mild Compression Deformity L1Document25 pagesA Case Study On Mild Compression Deformity L1JM UncianoNo ratings yet
- What Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistDocument12 pagesWhat Is Stroke?: BY: Luis Alberto Sanchez Hernandez Physical TherapistLidiaAMonroyRNo ratings yet
- Ineffective Cerebral Tissue Perfusion Related ToDocument7 pagesIneffective Cerebral Tissue Perfusion Related TohannahNo ratings yet
- Buerger's DiseaseDocument13 pagesBuerger's DiseaseJoan JuradoNo ratings yet
- Burns - Skin Integrity, ImpairedDocument2 pagesBurns - Skin Integrity, Impairedmakyofrancis20No ratings yet
- Avascular NecrosisDocument41 pagesAvascular NecrosisMohd Johari Mohd Shafuwan100% (1)
- Era University College of Nursing Lucknow: Submitted To-: Submitted byDocument7 pagesEra University College of Nursing Lucknow: Submitted To-: Submitted byAru Verma100% (1)
- Diabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40Document20 pagesDiabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40HUSSAIN NAZEESHANo ratings yet
- General Pathophysiology: Predisposing Factors: Precipitating FactorsDocument2 pagesGeneral Pathophysiology: Predisposing Factors: Precipitating FactorsIrish Nicole DCNo ratings yet
- HNPDocument7 pagesHNPLyka Mae Imbat - Pacnis100% (1)
- PPPDocument3 pagesPPPJack BangcoyoNo ratings yet
- Hemothorax HandoutsDocument2 pagesHemothorax HandoutsJunathan L. DelgadoNo ratings yet
- Head Injury....Document47 pagesHead Injury....nikowareNo ratings yet
- Tractions in OrthopaedicsDocument132 pagesTractions in Orthopaedicssiddhartha100% (1)
- Bell - S PalsyDocument17 pagesBell - S PalsyRickzen Hawkins NikecholantNo ratings yet
- Pott's DiseaseDocument30 pagesPott's DiseaseBipin SolankiNo ratings yet
- Spinal Cord Injury: Mrs. Zaida ZaracenaDocument36 pagesSpinal Cord Injury: Mrs. Zaida ZaracenaArdhel LoslosoNo ratings yet
- Potts Report KoDocument6 pagesPotts Report Kobsn2011No ratings yet
- CraniotomyDocument8 pagesCraniotomySyed AbudaheerNo ratings yet
- NCPDocument3 pagesNCPErica Denice CastilloNo ratings yet
- OsteomyelitisDocument15 pagesOsteomyelitisJayvee Ampo100% (2)
- Hemorrhagic StrokeDocument12 pagesHemorrhagic StrokeManggara Surya DharmaNo ratings yet
- SyncopeDocument28 pagesSyncopeDurgesh PushkarNo ratings yet
- ICU Case PresentationDocument51 pagesICU Case Presentationdeliejoyce0% (1)
- CVA IntroductionDocument12 pagesCVA IntroductionSuzette Rae TateNo ratings yet
- Pathophysiology of Head TraumaDocument12 pagesPathophysiology of Head TraumaMohammad ZianuddinNo ratings yet
- Spinal Cord InjuryDocument91 pagesSpinal Cord InjuryPrabaningrum DwidjoasmoroNo ratings yet
- Cerebral Concussion (Mini Case Study)Document8 pagesCerebral Concussion (Mini Case Study)Airalyn Chavez AlaroNo ratings yet
- Head Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingDocument31 pagesHead Injury: Manali H. Solanki F.Y. M.Sc. Nursing J G College of NursingWaqar AhmedNo ratings yet
- Pathophysiology of Brain Abscess Secondary To Chronic Otitis MediaDocument5 pagesPathophysiology of Brain Abscess Secondary To Chronic Otitis Mediafufulabrador100% (1)
- A Simple Guide to Cerebral Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Cerebral Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Spinal Cord Injuries Anatomy & Pathophysiology: JckingDocument51 pagesSpinal Cord Injuries Anatomy & Pathophysiology: JckingSatyaRandyNo ratings yet
- 1 Materi Kuliah Spine, Dr. AzharuddinDocument59 pages1 Materi Kuliah Spine, Dr. AzharuddinfazliahNo ratings yet
- Lecture 6 Spinal Cord InjuriesDocument26 pagesLecture 6 Spinal Cord InjuriesMahroosh KhanNo ratings yet
- Spinal Cord and Head InjuryDocument31 pagesSpinal Cord and Head InjuryRiris SutrisnoNo ratings yet
- Clinical Anatomy, Trauma of The Upper ExDocument103 pagesClinical Anatomy, Trauma of The Upper ExNeil Vincent De AsisNo ratings yet
- SCI (Spinal Cord Injury)Document51 pagesSCI (Spinal Cord Injury)Awal AlfitriNo ratings yet
- Spinal Cord InjuriesDocument31 pagesSpinal Cord Injuriesmariam bassemNo ratings yet
- Project File On Human Health and Disease.Document21 pagesProject File On Human Health and Disease.Sanampreet88% (34)
- Coding ZupkoDocument8 pagesCoding Zupkoashwanirana09No ratings yet
- Hydro Treatments TariffsDocument2 pagesHydro Treatments TariffsLouvern MoodleyNo ratings yet
- Commission On Higher Education Ched Memorandum Order NO. 30 Series of 2001 Subject: Updated Policies and Standards For Nursing EducationDocument34 pagesCommission On Higher Education Ched Memorandum Order NO. 30 Series of 2001 Subject: Updated Policies and Standards For Nursing EducationAngela SweetNo ratings yet
- Diabetes Mellitus: Specialty Icd 10 Icd 9-Cm Medlineplus Emedicine Patient Uk MeshDocument2 pagesDiabetes Mellitus: Specialty Icd 10 Icd 9-Cm Medlineplus Emedicine Patient Uk MeshMidaSimamoraNo ratings yet
- Hemotherapy: Pharma Lec. 1Document7 pagesHemotherapy: Pharma Lec. 1Ahmed Fittoh MosallamNo ratings yet
- Pulmonary Diseases Caused by Non-Tuberculous MycobacteriaDocument13 pagesPulmonary Diseases Caused by Non-Tuberculous MycobacteriaAdel HamadaNo ratings yet
- Tibial Plateau Fractures: Yasser AlwabliDocument35 pagesTibial Plateau Fractures: Yasser AlwabliPin Han NaNo ratings yet
- Book PDFDocument186 pagesBook PDFLuis CcenchoNo ratings yet
- Advanced Ventilation ManagementDocument3 pagesAdvanced Ventilation ManagementAnka EremiaNo ratings yet
- Traumatic Hyphema PDFDocument10 pagesTraumatic Hyphema PDFPratiwi SimanNo ratings yet
- Basic Concepts and Principles in Therapeutic CounselingDocument28 pagesBasic Concepts and Principles in Therapeutic CounselingPVallNo ratings yet
- Soap Note Rubric NS5067P April 2018: Teaching and Learning 6, 516-526Document1 pageSoap Note Rubric NS5067P April 2018: Teaching and Learning 6, 516-526coldNo ratings yet
- Widya - Basic Lumbal Spine MriDocument31 pagesWidya - Basic Lumbal Spine MriPrabaningrum DwidjoasmoroNo ratings yet
- New England Journal Medicine: The ofDocument10 pagesNew England Journal Medicine: The ofmayracppNo ratings yet
- ExoticHandbook2 PDFDocument617 pagesExoticHandbook2 PDFAdam PratamaNo ratings yet
- Homeostasis QuestionsDocument9 pagesHomeostasis QuestionsJohn OsborneNo ratings yet
- 040133.Steinmetz-Materia Medica Vegetabilis I PDFDocument234 pages040133.Steinmetz-Materia Medica Vegetabilis I PDFMaz RiezNo ratings yet
- Friedberg Wilt 2010 CT and MetaphorsDocument16 pagesFriedberg Wilt 2010 CT and MetaphorsAlexandra HuhNo ratings yet
- Choose Correct Answers:: A. Parotid Space InfectionDocument16 pagesChoose Correct Answers:: A. Parotid Space InfectionMohamed AhmedNo ratings yet
- Infusi IV RevDocument34 pagesInfusi IV RevNovi ArthaNo ratings yet
- Types of DiathermyDocument5 pagesTypes of DiathermyPavitra MurugesanNo ratings yet
- PRADEEP'S - Brain TumorDocument32 pagesPRADEEP'S - Brain TumorPRADEEPNo ratings yet
- Cox TechniqueDocument9 pagesCox TechniquemyokamaltaNo ratings yet