You might also like
- Skin Diseases Disorders ConditionsDocument104 pagesSkin Diseases Disorders ConditionsJerilee SoCute WattsNo ratings yet
- PDFDocument64 pagesPDFJerilee SoCute WattsNo ratings yet
- SkinDocument43 pagesSkinFhen Farrel100% (1)
- The HeartDocument42 pagesThe HeartJerilee SoCute WattsNo ratings yet
- The Circulatory System-: TransportDocument13 pagesThe Circulatory System-: TransportJerilee SoCute WattsNo ratings yet
- Digestive SystemDocument48 pagesDigestive SystemJerilee SoCute WattsNo ratings yet
- Urinary SystemDocument105 pagesUrinary SystemJerilee SoCute WattsNo ratings yet
- The Digestive System EssayDocument3 pagesThe Digestive System EssayJerilee SoCute Watts0% (1)
- Respiratory Centers of The BrainDocument36 pagesRespiratory Centers of The BrainJerilee SoCute WattsNo ratings yet
- The Digestive System: Cont'd (From Swallowing)Document56 pagesThe Digestive System: Cont'd (From Swallowing)Jerilee SoCute WattsNo ratings yet
- Reproductive SystemDocument80 pagesReproductive SystemJerilee SoCute WattsNo ratings yet
- The Conducting System of The HeartDocument37 pagesThe Conducting System of The HeartJerilee SoCute WattsNo ratings yet
- The Lymphatic SystemDocument50 pagesThe Lymphatic SystemJerilee SoCute Watts100% (1)
- The Digestive System Part 1Document28 pagesThe Digestive System Part 1Jerilee SoCute WattsNo ratings yet
- Respiration System PP TDocument57 pagesRespiration System PP Troyanirudh99No ratings yet
- Lecture 21 - Respiratory SystemDocument59 pagesLecture 21 - Respiratory SystemSkyBirdNo ratings yet
- Reproduction and DevelopmentDocument53 pagesReproduction and DevelopmentJerilee SoCute WattsNo ratings yet
- Reproductive System DisordersDocument62 pagesReproductive System DisordersJerilee SoCute Watts100% (2)
- Review Questions - HeartDocument1 pageReview Questions - HeartJerilee SoCute WattsNo ratings yet
- Human ReproductionDocument42 pagesHuman ReproductionAliDarimiKRNo ratings yet
- Pulmonary and Systemic CircuitsDocument38 pagesPulmonary and Systemic CircuitsJerilee SoCute WattsNo ratings yet
- Respiratory System 1Document29 pagesRespiratory System 1Jerilee SoCute WattsNo ratings yet
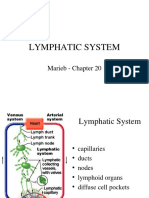
- Lymphatic System: Marieb Chapter 20Document22 pagesLymphatic System: Marieb Chapter 20Jerilee SoCute WattsNo ratings yet
- Unit 6 OsmolarityDocument59 pagesUnit 6 Osmolaritykrystal1994No ratings yet
- Lecture 2 Cardiovascular SystemDocument70 pagesLecture 2 Cardiovascular SystemJerilee SoCute WattsNo ratings yet
- Reproduction Summary NotesDocument16 pagesReproduction Summary NotesJerilee SoCute WattsNo ratings yet
- Reproduction NotesDocument20 pagesReproduction NotesMario BaemamentengNo ratings yet
- Lecture 1 Cardiovascular SystemDocument70 pagesLecture 1 Cardiovascular SystemJerilee SoCute WattsNo ratings yet
- Platelets and HemostasisDocument19 pagesPlatelets and HemostasisJerilee SoCute WattsNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Respiratory Examination (Updated Dec 21. JMS)Document39 pagesRespiratory Examination (Updated Dec 21. JMS)Shan PatelNo ratings yet
- Respiratory Care ModalitiesDocument101 pagesRespiratory Care ModalitiesIrish Jane GalloNo ratings yet
- StridorDocument20 pagesStridortkeat_9No ratings yet
- Tracheal Stenosis. - Evaluation of An Institutional Protocol and Introduction of Novel Surgical Criteria and Scoring System, 2019Document7 pagesTracheal Stenosis. - Evaluation of An Institutional Protocol and Introduction of Novel Surgical Criteria and Scoring System, 2019Araceli BarreraNo ratings yet
- Management of Elective LaryngectomyDocument6 pagesManagement of Elective LaryngectomyKj BrionesNo ratings yet
- Reviewer For Management of Common IllnessDocument27 pagesReviewer For Management of Common Illnessmarie vennis hamchawanNo ratings yet
- Science: Quarter 1 - Module 1: Respiratory and Circulatory Systems, Working With Other Organ SystemsDocument27 pagesScience: Quarter 1 - Module 1: Respiratory and Circulatory Systems, Working With Other Organ SystemsSofia Rose Saniel Gonzales100% (1)
- Tracheo BronchomalaciaDocument2 pagesTracheo BronchomalaciaSamah SuhailNo ratings yet
- Short Case-StnDocument26 pagesShort Case-StnSagarRathodNo ratings yet
- Imaging Evaluation of Tracheobronchial InjuriesDocument14 pagesImaging Evaluation of Tracheobronchial InjuriesSantiago TapiaNo ratings yet
- Lecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMDocument53 pagesLecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMlilimanao86% (7)
- Analgesia and Anesthesia in BirdDocument51 pagesAnalgesia and Anesthesia in BirdCynthia GonzalezNo ratings yet
- PropositionDocument38 pagesPropositionNaina ParasharNo ratings yet
- Akash Full Bio PDFDocument82 pagesAkash Full Bio PDFAdvik Sankar100% (1)
- IMCI CARE OF THE CHILD Topic 2Document10 pagesIMCI CARE OF THE CHILD Topic 2Hanna Evidente BakalNo ratings yet
- Our Lady of Fatima UniversityDocument5 pagesOur Lady of Fatima UniversityEmmanuel De LeonNo ratings yet
- Anatomy and Physiology of The Respiratory SystemDocument3 pagesAnatomy and Physiology of The Respiratory SystemLyka100% (1)
- DLP Gas Exchange in Plants and Animals - Q4 WK4 COT SAN CARLOS DIVISIONDocument8 pagesDLP Gas Exchange in Plants and Animals - Q4 WK4 COT SAN CARLOS DIVISIONjulzhaide100% (1)
- The Respiratory System PDFDocument25 pagesThe Respiratory System PDFbilly sauraNo ratings yet
- A Case Study On Bronchial Asthma in Acute ExacerbationDocument71 pagesA Case Study On Bronchial Asthma in Acute ExacerbationATEHAN BORDSNo ratings yet
- Bronco Pulmonary SegmentDocument24 pagesBronco Pulmonary SegmentAnkit PancholiNo ratings yet
- Body Systems ReviewDocument19 pagesBody Systems ReviewJ15No ratings yet
- Q4 STEM General Biology 2 Week 3Document4 pagesQ4 STEM General Biology 2 Week 3ralphNo ratings yet
- Medical Terminology, Chapter 3 ReviewDocument5 pagesMedical Terminology, Chapter 3 ReviewGregg ProducerNo ratings yet
- Trachea, Bronchial Tree and Bronchopulmonary Segments: by Nitisha GuptaDocument15 pagesTrachea, Bronchial Tree and Bronchopulmonary Segments: by Nitisha GuptaNITISHA GUPTANo ratings yet
- Anatomy and Physiology of Respiratory System Relevant To AnaesthesiaDocument10 pagesAnatomy and Physiology of Respiratory System Relevant To AnaesthesiaAnonymous h0DxuJTNo ratings yet
- Stridor Slides 2003 1231Document41 pagesStridor Slides 2003 1231entsrmcNo ratings yet
- Anesthesia For Patients With Thyroid Disease - UpToDateDocument12 pagesAnesthesia For Patients With Thyroid Disease - UpToDateJavier GlezqNo ratings yet
- Casestudy CAPDocument126 pagesCasestudy CAPArvin John Manuel100% (1)
- Case Study On Pulmonary TuberculosisDocument12 pagesCase Study On Pulmonary TuberculosisKirstie Claire100% (1)