You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Oral and Maxillofacial Medicine The Basi PDFDocument436 pagesOral and Maxillofacial Medicine The Basi PDFNimas Putri100% (2)
- Skin Premalignant and TumorsDocument95 pagesSkin Premalignant and TumorsmedicoprakashNo ratings yet
- For Mucocele Lesions - Careful Excisional BiopsyDocument11 pagesFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNo ratings yet
- Curriculum Vitae: Personal DetailsDocument3 pagesCurriculum Vitae: Personal DetailsBibek RajNo ratings yet
- QDWPlicDocument2 pagesQDWPlicBibek RajNo ratings yet
- JdsmcxnksDocument32 pagesJdsmcxnksBibek RajNo ratings yet
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDocument73 pagesInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNo ratings yet
- When Is Oral Biopsy Not Needed?Document6 pagesWhen Is Oral Biopsy Not Needed?Bibek RajNo ratings yet
- 3 UhnjkcDocument8 pages3 UhnjkcBibek RajNo ratings yet
- JDJDJDJDocument23 pagesJDJDJDJBibek RajNo ratings yet
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Document5 pagesBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNo ratings yet
- DhdifogkDocument4 pagesDhdifogkBibek RajNo ratings yet
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocument6 pagesVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNo ratings yet
- Trapezoidal Flap. A Diagrammatic IllustrationDocument6 pagesTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNo ratings yet
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocument3 pagesPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNo ratings yet
- DrtfygbyuijDocument29 pagesDrtfygbyuijBibek RajNo ratings yet
- FfghhthjgvyujhDocument1 pageFfghhthjgvyujhBibek RajNo ratings yet
- YuybnunhhuhbDocument2 pagesYuybnunhhuhbBibek RajNo ratings yet
- YudsbhcjDocument1 pageYudsbhcjBibek RajNo ratings yet
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocument1 pageBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNo ratings yet
- Dental Anxiety Form 4 PDFDocument2 pagesDental Anxiety Form 4 PDFBibek RajNo ratings yet
- Background Methods: Review' (OHAR) Guidance in BriefDocument1 pageBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNo ratings yet
- VfyggdbDocument33 pagesVfyggdbBibek RajNo ratings yet
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocument2 pagesUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNo ratings yet
- Rapid: Reducing Antibiotic Prescribing in DentistryDocument5 pagesRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNo ratings yet
- Warfarin and Your Dental Treatment: Information For PatientsDocument5 pagesWarfarin and Your Dental Treatment: Information For PatientsBibek RajNo ratings yet
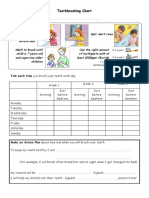
- Toothbrushing Chart PDFDocument1 pageToothbrushing Chart PDFBibek RajNo ratings yet
- TG 6 YhunjDocument48 pagesTG 6 YhunjBibek RajNo ratings yet
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocument1 pageToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNo ratings yet
- Oral PathologyDocument31 pagesOral PathologyAnasthasia hutagalungNo ratings yet
- Upper GI Disorders Study GuideDocument10 pagesUpper GI Disorders Study Guidemelpietrowski100% (1)
- Oral Squamous Cell Carcinoma Epidemiology ClinicalDocument7 pagesOral Squamous Cell Carcinoma Epidemiology Clinicalhtpxol1No ratings yet
- INTRODUCTIONDocument43 pagesINTRODUCTIONNikita NishanNo ratings yet
- (Edited) Reporting Oral Lesions (Group 6)Document53 pages(Edited) Reporting Oral Lesions (Group 6)Alexa AbrenicaNo ratings yet
- Head and Neck CancersDocument41 pagesHead and Neck CancersskhananiNo ratings yet
- CytologyDocument12 pagesCytologyEsther HutagalungNo ratings yet
- Carcinoma Buccal Mucosa: Dr. Abhilash G JR-3Document47 pagesCarcinoma Buccal Mucosa: Dr. Abhilash G JR-3LingeshNo ratings yet
- Management of Oral Leukoplakia - Analysis of The Literature: Material and MethodsDocument10 pagesManagement of Oral Leukoplakia - Analysis of The Literature: Material and MethodsyunisaNo ratings yet
- Lip CancerDocument4 pagesLip CancerSaman SadeghiNo ratings yet
- Description of Oral LesionsDocument6 pagesDescription of Oral LesionsVanshika JainNo ratings yet
- Oral Manifestations of Systemic DiseasesDocument14 pagesOral Manifestations of Systemic Diseasesshygal1981No ratings yet
- ENT MCQS (Ear, Pharynx, Tonsils, Deep Neck Infections, Oral Cavity)Document88 pagesENT MCQS (Ear, Pharynx, Tonsils, Deep Neck Infections, Oral Cavity)sidsudp75% (4)
- A Guide To Clinical Differential Diagnosis of Oral Mucosal LesionDocument46 pagesA Guide To Clinical Differential Diagnosis of Oral Mucosal LesionFasmiya ShariffNo ratings yet
- Skin CancerDocument215 pagesSkin CancerStefan CretuNo ratings yet
- Osmf-Classification Systems PDFDocument6 pagesOsmf-Classification Systems PDFporkodi sudhaNo ratings yet
- IJRRMS Vol.3 (4) - 21Document3 pagesIJRRMS Vol.3 (4) - 21mirabelladonnaNo ratings yet
- Oral Manifestation of AIDSDocument38 pagesOral Manifestation of AIDSoureducation.in100% (1)
- Derma BriefDocument7 pagesDerma BriefjeharatNo ratings yet
- Question:Discuss Various Malignancies of The Oral Region AnswersDocument6 pagesQuestion:Discuss Various Malignancies of The Oral Region AnswersMahdaba sheikh MohamudNo ratings yet
- 139 Case ReportDocument2 pages139 Case ReportlistyNo ratings yet
- Oral Speckled LeukoplakiaDocument3 pagesOral Speckled LeukoplakiaAnita PrastiwiNo ratings yet
- Current Concepts in Preventive Dentistry: Connie Myers Kracher, PHD (C), MSD, CdaDocument28 pagesCurrent Concepts in Preventive Dentistry: Connie Myers Kracher, PHD (C), MSD, CdalaykblakNo ratings yet
- Diseases of The Digestive SystemDocument37 pagesDiseases of The Digestive Systemrica ratnaNo ratings yet
- White Tongue & Thrush - Symptoms, Causes, TreatmentsDocument4 pagesWhite Tongue & Thrush - Symptoms, Causes, TreatmentsMudassar SattarNo ratings yet
- Oral CancerDocument29 pagesOral CancerBijen LangpoklakpamNo ratings yet
- Oral Medicine & RadioDocument25 pagesOral Medicine & RadioSree Harsha GunneriNo ratings yet
- КРАТКИЙ КУРС ПАТОМОРФОЛОГИИ ЧАСТЬ 1 ENGDocument214 pagesКРАТКИЙ КУРС ПАТОМОРФОЛОГИИ ЧАСТЬ 1 ENGRishik RanaNo ratings yet