You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Kementerian Riset Teknologi Dan Pendidikan TinggiDocument8 pagesKementerian Riset Teknologi Dan Pendidikan TinggiBella AndrianiNo ratings yet
- K5 - Metabolic SyndromeDocument32 pagesK5 - Metabolic SyndromeBella AndrianiNo ratings yet
- Microsoft PowerPoint - Integumentary System 2Document47 pagesMicrosoft PowerPoint - Integumentary System 2Cesar BucasasNo ratings yet
- K5 - Metabolic SyndromeDocument32 pagesK5 - Metabolic SyndromeBella AndrianiNo ratings yet
- Kumpulan SMART SOLUTION Mathematics by Mubarak SpentwoDocument43 pagesKumpulan SMART SOLUTION Mathematics by Mubarak SpentwoRizki EkoNo ratings yet
- K15 - IhdDocument23 pagesK15 - IhdRaka Notgoing Anywherebut AlwayseverywhereNo ratings yet
- JNC 8Document14 pagesJNC 8amiwahyuniNo ratings yet
- Fisiologi Integrative Functions Bshb14Document67 pagesFisiologi Integrative Functions Bshb14Bella AndrianiNo ratings yet
- Fisiologi Integrative Functions Bshb14Document67 pagesFisiologi Integrative Functions Bshb14Bella AndrianiNo ratings yet
- Fisiologi-The Autonomic Nervous System-Bshb14Document81 pagesFisiologi-The Autonomic Nervous System-Bshb14Bella AndrianiNo ratings yet
- Diagnosis Dan Penatalaksanaan Artritis ReumatoidDocument40 pagesDiagnosis Dan Penatalaksanaan Artritis ReumatoidBella AndrianiNo ratings yet
- Fisiologi-The Spinal Cord and Spinal Nerves-Bshb14Document51 pagesFisiologi-The Spinal Cord and Spinal Nerves-Bshb14Bella Andriani100% (1)
- K29 - Farmakologi AdrenalDocument38 pagesK29 - Farmakologi AdrenalBella AndrianiNo ratings yet
- Patologi Endokrin Edit BaruDocument32 pagesPatologi Endokrin Edit BaruBella AndrianiNo ratings yet
- Vital SignsDocument32 pagesVital SignsBella Andriani100% (1)
- Higher Algebra - Hall & KnightDocument593 pagesHigher Algebra - Hall & KnightRam Gollamudi100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Case PresentationDocument138 pagesCase PresentationrinlopenaiNo ratings yet
- Pre, Intra and Post Operative Nursing Management: Dr. Mohamed IdrissDocument37 pagesPre, Intra and Post Operative Nursing Management: Dr. Mohamed IdrissBsoom .iNo ratings yet
- Yoga in Pregnancy An Examination of Maternal And.19Document5 pagesYoga in Pregnancy An Examination of Maternal And.19SNFauziaNo ratings yet
- Paleracio Case StudyDocument18 pagesPaleracio Case StudySONY MANDAPNo ratings yet
- 2 Nursing Care PlanDocument1 page2 Nursing Care PlanPauline AnesNo ratings yet
- Non Verbal Pain Scale RevisedDocument9 pagesNon Verbal Pain Scale RevisedApriliana RatnaningrumNo ratings yet
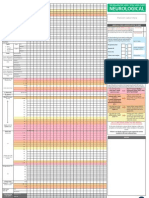
- Adult Early Warning Score Observation Chart For Neurosurgical UnitDocument1 pageAdult Early Warning Score Observation Chart For Neurosurgical UnitalexipsNo ratings yet
- General Physical ExaminationDocument18 pagesGeneral Physical ExaminationNick JacobNo ratings yet
- Nursing Care Plan - FeverDocument2 pagesNursing Care Plan - FeverRhelina MinNo ratings yet
- Uterine Atony - NCPDocument17 pagesUterine Atony - NCPMonica BorjaNo ratings yet
- PATCAREDocument39 pagesPATCAREVince Casugbo100% (1)
- Abstrak Nadia SariDocument2 pagesAbstrak Nadia SariDwi PratiwiNo ratings yet
- ICU Nursing L5Document78 pagesICU Nursing L5MaxNo ratings yet
- Case Presentation FormatDocument4 pagesCase Presentation Formatdeliciouslyme0688% (8)
- Using A Cooling BlanketDocument2 pagesUsing A Cooling BlanketydtrgnNo ratings yet
- Burn NCPDocument4 pagesBurn NCPYvesNo ratings yet
- Abdominal Pain ManagementDocument50 pagesAbdominal Pain ManagementGI SanadaNo ratings yet
- Fundamentals of Nursing and Nursing Health Assessment Question BankDocument126 pagesFundamentals of Nursing and Nursing Health Assessment Question BankCas Tan100% (1)
- A Narrative Report On: Physical AssesmentDocument11 pagesA Narrative Report On: Physical AssesmentchelseyNo ratings yet
- IPED2015CS01 MAC049 PIS&ICF 4.0 Part A and B (18dec2018) - Final VersionDocument24 pagesIPED2015CS01 MAC049 PIS&ICF 4.0 Part A and B (18dec2018) - Final VersionASCRONo ratings yet
- Tourniquet Use at The Boston Marathon Bombing: Lost in TranslationDocument6 pagesTourniquet Use at The Boston Marathon Bombing: Lost in TranslationFabio Ferreira SaNo ratings yet
- Percakapan BHS Inggris Penerimaan PasienDocument5 pagesPercakapan BHS Inggris Penerimaan PasienYulia WyazztNo ratings yet
- Patient Assestment PDFDocument12 pagesPatient Assestment PDFAnonymous 85pLrRNo ratings yet
- CCM Study Guide Foundations of NursingDocument46 pagesCCM Study Guide Foundations of NursingAlexandra BrowneNo ratings yet
- NCP H-MoleDocument6 pagesNCP H-MoleJaysonPangilinanAban100% (3)
- Erni Purba COD 5Document10 pagesErni Purba COD 5andreNo ratings yet
- NCP On SahDocument21 pagesNCP On SahDr-Sanjay SinghaniaNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanMariel GamaloNo ratings yet
- LIPPNCOTT Vital Signs Height Weight Chapter 016Document72 pagesLIPPNCOTT Vital Signs Height Weight Chapter 016Sara SabraNo ratings yet
- Patient Assessment Patient Assessment PlanDocument3 pagesPatient Assessment Patient Assessment PlanKevin PadilloNo ratings yet