You might also like
- ABG InterpretationDocument31 pagesABG Interpretationɹǝʍdןnos100% (12)
- Denver II Test Form PDFDocument2 pagesDenver II Test Form PDFFiorellaBeatriz100% (4)
- Interpretation of Arterial Blood Gases (ABGs)Document6 pagesInterpretation of Arterial Blood Gases (ABGs)afalfitraNo ratings yet
- Arterial Blood Gas Analysis - making it easyFrom EverandArterial Blood Gas Analysis - making it easyRating: 4.5 out of 5 stars4.5/5 (4)
- Diabetic KetoacidosisDocument38 pagesDiabetic KetoacidosisAwatef AbushhiwaNo ratings yet
- Study Guide For OBGYNDocument34 pagesStudy Guide For OBGYNFiorellaBeatriz100% (1)
- Interpretasi AGDDocument129 pagesInterpretasi AGDIta SobaNo ratings yet
- Approach To Acid-Base Problems: DR Frank DalyDocument57 pagesApproach To Acid-Base Problems: DR Frank DalyscanutdNo ratings yet
- Presentation1 5, Acid-BaseDocument32 pagesPresentation1 5, Acid-BaseOliviaLaneNo ratings yet
- Interpreting ABG - An Interative Session: Dr. Manjunath Patil Professor, Dept. of Anaesthesiology J.N.Medical CollegeDocument31 pagesInterpreting ABG - An Interative Session: Dr. Manjunath Patil Professor, Dept. of Anaesthesiology J.N.Medical CollegeMadhan Mohan Reddy KatikareddyNo ratings yet
- Blood Gas TestDocument6 pagesBlood Gas TestyudhafpNo ratings yet
- Laki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumDocument66 pagesLaki-Laki, 21 Tahun Dengan Ketoasidosis DiabetikumAnonymous gudRSKNo ratings yet
- ArpitDocument73 pagesArpitDurgesh PushkarNo ratings yet
- Michael Chansky Acid Base Made Easy HandoutDocument18 pagesMichael Chansky Acid Base Made Easy HandoutTeguh RamadhanNo ratings yet
- Acid Base Disorders: Hasan Al-Dorzi, MD Pulmonary and Critical Care Consultant, Intensive Care DepartmentDocument47 pagesAcid Base Disorders: Hasan Al-Dorzi, MD Pulmonary and Critical Care Consultant, Intensive Care DepartmentAmjaSaudNo ratings yet
- Metabolic Acidosis CasesDocument20 pagesMetabolic Acidosis CaseswiamNo ratings yet
- Blood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSIDocument39 pagesBlood Gases and Acid-Base Disorders: Dr. Wan Nedra Sp. A Pediatricts Departement University of YARSISalsabila RahmaNo ratings yet
- Saumya Gupta Moderator: Dr. Vishal GuptaDocument41 pagesSaumya Gupta Moderator: Dr. Vishal Guptaimranqazi11No ratings yet
- Abg Analysis & Acid-Base Disorders: DR - Anitha KsDocument24 pagesAbg Analysis & Acid-Base Disorders: DR - Anitha KsanithaNo ratings yet
- Acid-Base Disorders and The ABGDocument28 pagesAcid-Base Disorders and The ABGPaul KelnerNo ratings yet
- ABG Interpretation - ATSDocument5 pagesABG Interpretation - ATSHAMMYER ALROKHAMINo ratings yet
- Acid BaseDocument28 pagesAcid BaseDexter GabrielNo ratings yet
- Acid BaseDocument28 pagesAcid Basezendah1No ratings yet
- LRP CriticalCare Sample2Document46 pagesLRP CriticalCare Sample2Aniket ChoudharyNo ratings yet
- Hand Out 2 NCM 103 PrelimDocument3 pagesHand Out 2 NCM 103 PrelimLouisa Marie MirandaNo ratings yet
- Acid BaseDocument28 pagesAcid BaseSamantha DeshapriyaNo ratings yet
- Acid - Base Balance & Abg AnalysisDocument71 pagesAcid - Base Balance & Abg AnalysisMohan KrishnaNo ratings yet
- The Acid Base Balance: Faculty of Medicine Anesthesia and Intensive Care DepartmentDocument36 pagesThe Acid Base Balance: Faculty of Medicine Anesthesia and Intensive Care DepartmentCamelia A. ParuschiNo ratings yet
- Case Presentation NewDocument93 pagesCase Presentation NewYanesh BishundatNo ratings yet
- MedSurg Group2Document4 pagesMedSurg Group2Lacangan, Thea YvonneNo ratings yet
- Acid Base BalanceDocument45 pagesAcid Base BalanceSameer Ul BashirNo ratings yet
- BiochemistryDocument33 pagesBiochemistryamhhospital0No ratings yet
- Interpretation of Arterial Blood GasesDocument16 pagesInterpretation of Arterial Blood GasesRuby Ann Cañero HigoyNo ratings yet
- Acid Base Disorders JAPIDocument5 pagesAcid Base Disorders JAPIVitrag_Shah_1067No ratings yet
- Arterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPDocument39 pagesArterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPGio Tamaño BalisiNo ratings yet
- Arterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPDocument39 pagesArterial Blood Gas Interpretation: Joseph Brian L. Costiniano, MD, DPCPevbptrprnrmNo ratings yet
- ABG AnalysisDocument46 pagesABG Analysisregole100% (1)
- Kursus Critical Care Respiratory FunctionDocument63 pagesKursus Critical Care Respiratory FunctionJeyaganesh SellvarajuNo ratings yet
- 128 Diabetic KetoacidosisDocument9 pages128 Diabetic KetoacidosisDite Bayu NugrohoNo ratings yet
- Assalamualaikum Wr. WBDocument19 pagesAssalamualaikum Wr. WBAmalia DefinaNo ratings yet
- ABG Algorithm PDFDocument2 pagesABG Algorithm PDFamin2014No ratings yet
- Acid-Base Made EasyDocument14 pagesAcid-Base Made EasyMayer Rosenberg100% (10)
- Clinical Education: Interpretation of AbgsDocument8 pagesClinical Education: Interpretation of AbgsRumela Ganguly ChakrabortyNo ratings yet
- Acid BaseDocument81 pagesAcid Basenader siamNo ratings yet
- Arterial Blood Gases: Mike Runyon, MD July 15, 2010Document46 pagesArterial Blood Gases: Mike Runyon, MD July 15, 2010mamiraliNo ratings yet
- ABG MMHG InterpretationDocument92 pagesABG MMHG InterpretationManmeet SNo ratings yet
- Pleno Minggu 2 Blok 3.4Document84 pagesPleno Minggu 2 Blok 3.4Devi Yunita PurbaNo ratings yet
- "Blood Gas Analysis in A Nutshell: DR Anshuman MishraDocument28 pages"Blood Gas Analysis in A Nutshell: DR Anshuman MishraMinaz PatelNo ratings yet
- Interpretation of Arterial Blood GasesDocument7 pagesInterpretation of Arterial Blood GasesGaby FernándezNo ratings yet
- Acid Base PhysiologyDocument4 pagesAcid Base PhysiologyGhadeer EbraheemNo ratings yet
- Arterial Blood GasDocument48 pagesArterial Blood GaslovianettesherryNo ratings yet
- ABG AnalysisDocument22 pagesABG Analysisrajan40dmcNo ratings yet
- Arterial Blood Gas InterpretationsDocument7 pagesArterial Blood Gas InterpretationsErin TraversNo ratings yet
- Cases Acid BaseDocument3 pagesCases Acid BaseSa MoNo ratings yet
- Interpretation of Arterial Blood Gases (Abgs) I David A. Kaufman, MD DDocument17 pagesInterpretation of Arterial Blood Gases (Abgs) I David A. Kaufman, MD DingridpuspitaNo ratings yet
- Arterial Blood Gas (Abg)Document10 pagesArterial Blood Gas (Abg)Kita kitaNo ratings yet
- Arterial Blood GasDocument55 pagesArterial Blood GasRathis Dasan100% (1)
- Blood Gas AnalysisDocument39 pagesBlood Gas Analysisjtalan9No ratings yet
- Diagnostic Tests GosayeDocument188 pagesDiagnostic Tests GosayeAbdii TolasaNo ratings yet
- Acid-Base Balance 2Document62 pagesAcid-Base Balance 2chimbimbNo ratings yet
- Acid Base Imbalance 2Document26 pagesAcid Base Imbalance 2Female calmNo ratings yet
- Metabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandMetabolic Alkalosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- ABA ProvidersDocument2 pagesABA ProvidersFiorellaBeatrizNo ratings yet
- Milestone MomentsDocument60 pagesMilestone MomentsFiorellaBeatrizNo ratings yet
- Introduction To Laboratory Tests Handout VersionDocument58 pagesIntroduction To Laboratory Tests Handout VersionFiorellaBeatrizNo ratings yet
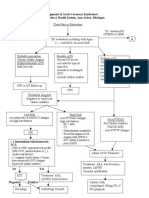
- Management of Acute Coronary Syndromes St. Joseph Mercy Health System, Ann Arbor, MichiganDocument2 pagesManagement of Acute Coronary Syndromes St. Joseph Mercy Health System, Ann Arbor, MichiganFiorellaBeatrizNo ratings yet
- FMStudent OME VideoGuideForFMDocument4 pagesFMStudent OME VideoGuideForFMFiorellaBeatriz100% (1)
- American Academy of Pediatrics and American Academy of Family PhysiciansDocument17 pagesAmerican Academy of Pediatrics and American Academy of Family PhysiciansFiorellaBeatrizNo ratings yet
- CSDCDocument5 pagesCSDCFiorellaBeatrizNo ratings yet
- CYW ACEQ UserGuideDocument21 pagesCYW ACEQ UserGuideFiorellaBeatrizNo ratings yet
- 552.full DisparitiesDocument4 pages552.full DisparitiesFiorellaBeatrizNo ratings yet
- Arterial Blood Gas InterpretationsDocument7 pagesArterial Blood Gas InterpretationsErin TraversNo ratings yet
- Ketosis DMDocument33 pagesKetosis DMtiaNo ratings yet
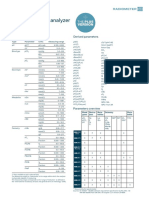
- MAPSSS000188 R2 ABL800 FLEX PLUS Specs - EN - LowDocument2 pagesMAPSSS000188 R2 ABL800 FLEX PLUS Specs - EN - LowmemddrNo ratings yet
- Alcoholic KetoacidosisDocument3 pagesAlcoholic KetoacidosisFaishal HanifNo ratings yet
- Diabetic Ketoacidosis CQBDocument9 pagesDiabetic Ketoacidosis CQBkajanyloganNo ratings yet
- Nephrology & Urology: Archer Online USMLE ReviewsDocument107 pagesNephrology & Urology: Archer Online USMLE ReviewsBeerappaJanpetNo ratings yet
- Acid Base Balance OR OR Regulation of Blood PHDocument175 pagesAcid Base Balance OR OR Regulation of Blood PHhirendra patel100% (1)
- DAHİLİYE'DETUS SORULARI Eng PDFDocument83 pagesDAHİLİYE'DETUS SORULARI Eng PDFKhalid ShafiqNo ratings yet
- Acid Base Balance Pathophysiology NursingDocument7 pagesAcid Base Balance Pathophysiology Nursinggrad_nurse_2015100% (2)
- Anionic GapDocument8 pagesAnionic GapMaria-Larisa HohanNo ratings yet
- Unmeasured Anions Identified by The Fencl-Stewart Method Predict Mortality Better Than Base Excess, Anion Gap, and Lactate in Patients in The Pediatric Intensive Care Unit.Document11 pagesUnmeasured Anions Identified by The Fencl-Stewart Method Predict Mortality Better Than Base Excess, Anion Gap, and Lactate in Patients in The Pediatric Intensive Care Unit.Defranky TheodorusNo ratings yet
- Applications of The Henderson Hasselbalch EquationDocument8 pagesApplications of The Henderson Hasselbalch EquationSittie Fahieda AloyodanNo ratings yet
- EMERGENCIES IN DM (KAD Dan HHS)Document26 pagesEMERGENCIES IN DM (KAD Dan HHS)ozNo ratings yet
- Karapitiya OSCE 2017 With AnswersDocument34 pagesKarapitiya OSCE 2017 With Answersweerawarna fernandoNo ratings yet
- AcidoBaseDrKellum PDFDocument84 pagesAcidoBaseDrKellum PDFalexander197100% (1)
- Komplikasi Akut DM - Dr. RensaDocument42 pagesKomplikasi Akut DM - Dr. RensaLeonardus William KuswaraNo ratings yet
- Slide Kuliah Gagal Nafas-AgdDocument78 pagesSlide Kuliah Gagal Nafas-Agdeko andryNo ratings yet
- Fluid & Acid Base Mcqs From Harrison 17 EditionDocument9 pagesFluid & Acid Base Mcqs From Harrison 17 Editionatul_desai_3No ratings yet
- How To Interpret Arterial Blood Gas Data?Document7 pagesHow To Interpret Arterial Blood Gas Data?Karoline MenezesNo ratings yet
- Arterial Blood Gas Case Questions and AnswersDocument7 pagesArterial Blood Gas Case Questions and AnswersWaqas QureshiNo ratings yet
- RTA Types NidisaaDocument16 pagesRTA Types NidisaaNidisaaNo ratings yet
- Acid Base BalanceDocument13 pagesAcid Base BalanceRashed ShatnawiNo ratings yet
- Clinical Assessment of Acid-Base Status: Comparison of The Henderson-Hasselbalch and Strong Ion ApproachesDocument14 pagesClinical Assessment of Acid-Base Status: Comparison of The Henderson-Hasselbalch and Strong Ion Approachesgarinda almadutaNo ratings yet
- Renal Tubular AcidosisDocument5 pagesRenal Tubular AcidosisVaio Wolff AbendrothNo ratings yet
- Arterial Blood Gases A Simplified Bedside Approach 2167 0897.1000153Document5 pagesArterial Blood Gases A Simplified Bedside Approach 2167 0897.1000153veerNo ratings yet
- Abg by DR Manna, Department of Emergency Medicine, Amrita Institute of Medical Sceinces, Kochi, KeralaDocument50 pagesAbg by DR Manna, Department of Emergency Medicine, Amrita Institute of Medical Sceinces, Kochi, KeralaAETCM Emergency medicine100% (1)
- Acid-Base Balance and DisodersDocument86 pagesAcid-Base Balance and DisodersPrincewill SeiyefaNo ratings yet
- V.I.P. Very Important Points: Dr. Adel Al HarbiDocument143 pagesV.I.P. Very Important Points: Dr. Adel Al HarbiSukainah AL-AbkaryNo ratings yet
- Case #1: Cases in Acid - Base DisturbanceDocument10 pagesCase #1: Cases in Acid - Base DisturbanceIsraa SalmanNo ratings yet
- Kalkulator AGDDocument2 pagesKalkulator AGDMuliaNo ratings yet