You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- S 015 Med GuideDocument3 pagesS 015 Med GuideEko YuliantoNo ratings yet
- Pharmacology of Antipyretic DrugsDocument19 pagesPharmacology of Antipyretic DrugsPretty HiaNo ratings yet
- Polmaforce RCPA Circular 16.10.23Document2 pagesPolmaforce RCPA Circular 16.10.23ALINo ratings yet
- List of Nationally Authorised Medicinal Products: Active Substance: Nimesulide (Systemic Formulations)Document7 pagesList of Nationally Authorised Medicinal Products: Active Substance: Nimesulide (Systemic Formulations)mcamilaarredondovelezNo ratings yet
- Vademecum Valesalud 201401Document42 pagesVademecum Valesalud 201401petacosNo ratings yet
- Data Stok Opname Obat Antisakit TabDocument25 pagesData Stok Opname Obat Antisakit TabSandiNo ratings yet
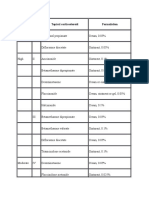
- Potency Class Topical Corticosteroid FormulationDocument5 pagesPotency Class Topical Corticosteroid FormulationgowindamijayaNo ratings yet
- NSAIDDocument5 pagesNSAIDAndrei CluNo ratings yet
- 2021 Update Management Pain (Dokter & Medical)Document30 pages2021 Update Management Pain (Dokter & Medical)Andri MuliaNo ratings yet
- Analgetik Non Opioid NsaidDocument3 pagesAnalgetik Non Opioid NsaidShintaNo ratings yet
- AseaDocument24 pagesAseaYahdian RasyadiNo ratings yet
- Ains RecomandariDocument2 pagesAins RecomandariBrîndușa PetruțescuNo ratings yet
- Steroid Potency ChartDocument1 pageSteroid Potency ChartKumar Bhai100% (2)
- Antiinflamatoare NesteroidieneDocument2 pagesAntiinflamatoare NesteroidieneLore DanaNo ratings yet
- Diuretics Antidiabetics AnalgesicsDocument7 pagesDiuretics Antidiabetics AnalgesicsBillQueNo ratings yet
- Antidepressant DrugsDocument10 pagesAntidepressant DrugsHazel Joy Galamay - GarduqueNo ratings yet
- Lista-OTC-25 11 2022Document54 pagesLista-OTC-25 11 2022ValeraNo ratings yet
- Activities of Ethanolic Extracts Piper Crocatum As Anti-Inflammatory in Male White Rat Strains Sprague-DawleyDocument9 pagesActivities of Ethanolic Extracts Piper Crocatum As Anti-Inflammatory in Male White Rat Strains Sprague-Dawleyseptodrasta123No ratings yet
- Invoice Februari OtwDocument43 pagesInvoice Februari OtwAnnissa Puspa JNo ratings yet
- Andhika Rezeky Gunawan - Tugas FarmakoDocument4 pagesAndhika Rezeky Gunawan - Tugas FarmakoAndhika gunawanNo ratings yet
- Catalogo Ampollas - F24 - BCV - 35.69$ 09-12-2023Document20 pagesCatalogo Ampollas - F24 - BCV - 35.69$ 09-12-2023Reimon NavaNo ratings yet
- Images: All Videos Books News Maps FlightsDocument1 pageImages: All Videos Books News Maps FlightsChan ParinaNo ratings yet
- Descripción PVF Xistencias: Desc%Document18 pagesDescripción PVF Xistencias: Desc%Nelly NoemiNo ratings yet
- Listado de Productos Eticos Serrano GomezDocument9 pagesListado de Productos Eticos Serrano GomezKelli VergelNo ratings yet
- 3 - NSAIDsDocument40 pages3 - NSAIDsJuan UmiwasNo ratings yet
- Original Article: BackgroundDocument4 pagesOriginal Article: BackgroundYuni IHNo ratings yet
- Rekap Obat January 2020Document19 pagesRekap Obat January 2020Liska PrahestikaNo ratings yet
- Medications To Avoid Before and After SurgeryDocument3 pagesMedications To Avoid Before and After SurgeryIoana PirvulescuNo ratings yet
- 2007 08/31 DR Gokhale DischargeDocument4 pages2007 08/31 DR Gokhale Dischargeapi-26176155No ratings yet
- ANTINYERIDocument12 pagesANTINYERINunuk HidayantiNo ratings yet