You might also like
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- HematologyDocument57 pagesHematologyNurhidayahNo ratings yet
- Case Analysis:: Myocardial InfarctionDocument76 pagesCase Analysis:: Myocardial InfarctionIpeNo ratings yet
- Pleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandPleural Effusion, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Cardiogenic Shock PDFDocument14 pagesCardiogenic Shock PDFAdreiTheTripleANo ratings yet
- Ischemic Heart DiseaseDocument116 pagesIschemic Heart DiseaseAndrew OrlovNo ratings yet
- Atelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesFrom EverandAtelectasis, (Lung Collapse) A Simple Guide To The Condition, Diagnosis, Treatment And Related DiseasesNo ratings yet
- Angina PectorisDocument38 pagesAngina Pectorisekhafagy100% (1)
- Liver Cirrhosis: Review HepatologyDocument71 pagesLiver Cirrhosis: Review HepatologyAstri Arri FebriantiNo ratings yet
- Assessment of Cardiovascular2014Document12 pagesAssessment of Cardiovascular2014alphabennydelta4468No ratings yet
- Myocardial InfarctionDocument23 pagesMyocardial InfarctionAnelle Umali50% (2)
- Azure Pipelines Building GitHub Repositories by Example - CodeProjectDocument11 pagesAzure Pipelines Building GitHub Repositories by Example - CodeProjectgfgomesNo ratings yet
- Chest PainDocument31 pagesChest PainMarwan GamaleldinNo ratings yet
- 1st, 2nd, 3rd Degree AV BLockDocument8 pages1st, 2nd, 3rd Degree AV BLockladydreamer_92No ratings yet
- Acute Myocardial InfarctionDocument67 pagesAcute Myocardial InfarctionJoshua Pascasio100% (1)
- Copd 200412082048Document139 pagesCopd 200412082048Richard ArceNo ratings yet
- DT 230 Manual PDFDocument102 pagesDT 230 Manual PDFCarlos ValenciaNo ratings yet
- Hypertensive Crisis: - Alexter John C. Fajardo M.DDocument49 pagesHypertensive Crisis: - Alexter John C. Fajardo M.DAlexter John Cabalonga FajardoNo ratings yet
- Physiological Regulation of Arterial Blood PressureDocument36 pagesPhysiological Regulation of Arterial Blood PressureFrancesNo ratings yet
- Acute Respiratory Distress SyndromeDocument77 pagesAcute Respiratory Distress SyndromeAnnisa Dyah ChairiniNo ratings yet
- Types Heart Failure PDFDocument10 pagesTypes Heart Failure PDFHannaNo ratings yet
- Asthma and CopdDocument44 pagesAsthma and CopdBeer Dilacshe100% (1)
- CardiomyopathyDocument2 pagesCardiomyopathyBianca SarmientoNo ratings yet
- Myocardial Infarction. BPTDocument62 pagesMyocardial Infarction. BPTAanchal GuptaNo ratings yet
- Valvular Heart DiseasesDocument29 pagesValvular Heart Diseasesbpt2No ratings yet
- Myocardial InfarctionDocument47 pagesMyocardial Infarctionsanjesh1100% (2)
- MF3 - Ischemic Heart DiseaseDocument28 pagesMF3 - Ischemic Heart DiseaseAnnbe BarteNo ratings yet
- Cerebrovascular AccidentDocument31 pagesCerebrovascular AccidentRam ReddyNo ratings yet
- Murugan Pictures Collection - 0 PDFDocument33 pagesMurugan Pictures Collection - 0 PDFsaurabh72303100% (3)
- CopdDocument74 pagesCopdSardor AnorboevNo ratings yet
- Diabetes MellitusDocument16 pagesDiabetes Mellitusirayo50% (2)
- Pulmonary Rehabilitation PPDocument19 pagesPulmonary Rehabilitation PPnashqonashNo ratings yet
- Ischemic Heart DiseaseDocument67 pagesIschemic Heart Diseasealfaz lakhani80% (5)
- Myocardial InfarctionDocument40 pagesMyocardial InfarctionHIRANGER100% (3)
- CopdDocument60 pagesCopdRizqy Shofianingrum100% (1)
- Diabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40Document20 pagesDiabetic Ketoacidosis: Presented by The Students From Roll Numbers 31 - 40HUSSAIN NAZEESHANo ratings yet
- Cerebrovascular Accident (Stroke, Brain Attack) : Click To Edit Master Subtitle StyleDocument21 pagesCerebrovascular Accident (Stroke, Brain Attack) : Click To Edit Master Subtitle StyleKatri ArasaNo ratings yet
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseaseABREHAM BUKULONo ratings yet
- Basic Veterinary Immunology - CallahanDocument350 pagesBasic Veterinary Immunology - CallahanNana0% (1)
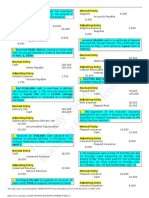
- Adjusting Entries FarDocument2 pagesAdjusting Entries FarKylha BalmoriNo ratings yet
- Syndrom of Consolidated Pulmonary Tissue. Pneumonia. Athelectasis. Andrei IchimDocument114 pagesSyndrom of Consolidated Pulmonary Tissue. Pneumonia. Athelectasis. Andrei IchimYan Sheng Ho100% (1)
- I. A. Brief Description: Chakinala, 2015)Document54 pagesI. A. Brief Description: Chakinala, 2015)Kacelyn QuibanNo ratings yet
- Hepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetDocument48 pagesHepatitis A-E Viruses: Ini PPT DR - Catur Dari InternetNurhidayahNo ratings yet
- ECG Changes in Drug and Electrolyte AbnormalitiesDocument28 pagesECG Changes in Drug and Electrolyte AbnormalitiesNachiket Vijay Potdar100% (1)
- Community Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCommunity Acquired Pneumonia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Best Stochastic Trading StrategyDocument5 pagesBest Stochastic Trading StrategyBadrun Ibrahim67% (3)
- Pulmonary EmbolismDocument96 pagesPulmonary Embolismsamice5100% (1)
- Cor Pulmonale: Dr. Gerrard UyDocument13 pagesCor Pulmonale: Dr. Gerrard Uyfaridah azzah sariNo ratings yet
- Pulmonary EdemaDocument10 pagesPulmonary EdemaMohammed EliasNo ratings yet
- Pulmonary HypertensionDocument63 pagesPulmonary HypertensionChrishan Shivanthan100% (4)
- Pathogenesis of Micro and Macrovascular Complications of DiabetesDocument4 pagesPathogenesis of Micro and Macrovascular Complications of DiabetesFrancesca LiNo ratings yet
- One Medical Overview Presenation - FINALDocument33 pagesOne Medical Overview Presenation - FINALNafiahNo ratings yet
- Intestinal Obstruction: Methas Arunnart MDDocument42 pagesIntestinal Obstruction: Methas Arunnart MDJhe-sie AngelinaNo ratings yet
- Pulmonary EmbolismDocument5 pagesPulmonary EmbolismNica Duco100% (2)
- Preview of Tyre Retreading PDFDocument20 pagesPreview of Tyre Retreading PDFLucky TraderNo ratings yet
- Bronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandBronchiectasis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Congestive Cardiac FailureDocument38 pagesCongestive Cardiac FailureSalman KhanNo ratings yet
- Early and Late Signs of Increased Intracranial PressureDocument8 pagesEarly and Late Signs of Increased Intracranial PressureRhae Raynog100% (2)
- Pulmonary EdemaDocument59 pagesPulmonary EdemamaibejoseNo ratings yet
- 1.1 Biology of Bone HealingDocument32 pages1.1 Biology of Bone HealingCristian CumpănăNo ratings yet
- Respiratory AcidosisDocument16 pagesRespiratory AcidosisIssa GutierrezNo ratings yet
- N24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis AsthmaDocument42 pagesN24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis Asthmadentist40No ratings yet
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric WongDocument7 pagesChronic Obstructive Pulmonary Disease (COPD) : Sultan Chaudhry Benny Dua Eric Wongjamil aldasriNo ratings yet
- Hyperglycemic Hyperosmolar StateDocument17 pagesHyperglycemic Hyperosmolar StateAqila Mumtaz50% (2)
- Coronary Artery Disease Cad2Document182 pagesCoronary Artery Disease Cad2Mamot MotNo ratings yet
- Acute Kidney InjuryDocument37 pagesAcute Kidney InjuryLani BuenaventuraNo ratings yet
- Hypovolemic ShockDocument13 pagesHypovolemic ShockJed ProwellNo ratings yet
- What Is Hypertensive NephropathyDocument11 pagesWhat Is Hypertensive NephropathyIvy Pamanian DeldaNo ratings yet
- Cardio-Vascular Disease: Mitral Stenosis & Mitral RegurgitationDocument25 pagesCardio-Vascular Disease: Mitral Stenosis & Mitral Regurgitationyulia silviNo ratings yet
- Respiration 16 Respiratory FailureDocument31 pagesRespiration 16 Respiratory Failureapi-19641337No ratings yet
- Tumor GinjalDocument63 pagesTumor GinjalNurhidayah100% (1)
- Pemeriksaan Laboratorium Pada Onkologi: Tissa Octavira Permatasari Fakultas Kedokteran Unswagati CirebonDocument7 pagesPemeriksaan Laboratorium Pada Onkologi: Tissa Octavira Permatasari Fakultas Kedokteran Unswagati CirebonNurhidayahNo ratings yet
- 1 Patofisiologi StrokeDocument20 pages1 Patofisiologi StrokeNurhidayahNo ratings yet
- Swine FluDocument22 pagesSwine FluNurhidayahNo ratings yet
- Fisiologi HepatobiliarDocument17 pagesFisiologi HepatobiliarNurhidayahNo ratings yet
- Lamborghini Project ReportDocument23 pagesLamborghini Project Reportprasad dadasaheb tupake100% (1)
- hw8 SolnsDocument9 pageshw8 SolnsJennyNo ratings yet
- Asme PTC 4.3 - 1968Document31 pagesAsme PTC 4.3 - 1968Tudorache CristianNo ratings yet
- 4a External GA RTU Typical For ASS - RSSDocument1 page4a External GA RTU Typical For ASS - RSSVinay GuptaNo ratings yet
- Monday Morning ArtDocument4 pagesMonday Morning ArtJuan Carlos PASQUEL G.No ratings yet
- Gentics Lab 5Document12 pagesGentics Lab 5Time NextNo ratings yet
- Absolute Judgement: IE-311 Ergonomics 2Document19 pagesAbsolute Judgement: IE-311 Ergonomics 2Lucky Gem AsibuqueNo ratings yet
- ISO#IEC 5055 2021 (E) - Character PDF Document (EN)Document7 pagesISO#IEC 5055 2021 (E) - Character PDF Document (EN)fogsaNo ratings yet
- Research Writing Series 6 How To Write An AbstractDocument20 pagesResearch Writing Series 6 How To Write An AbstractMaria Leira Calubayan Laurel0% (1)
- E PassbookDocument3 pagesE PassbookJASVINDER SINGHNo ratings yet
- The Angel ShipwreckDocument25 pagesThe Angel ShipwreckOctavio del RíoNo ratings yet
- Application New 2023Document8 pagesApplication New 2023SFS LOANSNo ratings yet
- ESAB Welding & Cu Ing Products: A515 516 4 In. Thick 2 In. Root GapDocument1 pageESAB Welding & Cu Ing Products: A515 516 4 In. Thick 2 In. Root Gapalok987No ratings yet
- ACMCOMM K31 - Ranillo, Eana - Critique PaperDocument1 pageACMCOMM K31 - Ranillo, Eana - Critique PaperEana RanilloNo ratings yet
- Managerial Accounting 5th Edition Wild Test BankDocument35 pagesManagerial Accounting 5th Edition Wild Test Bankwannesswoodsarehv0t06100% (28)
- DLL Perdev Week 8 - GuiangDocument13 pagesDLL Perdev Week 8 - GuiangAnne RiveroNo ratings yet
- Oral MATH 9Document2 pagesOral MATH 9Rizza Mae ReponteNo ratings yet
- Kez CondensadorasDocument40 pagesKez CondensadorasGerman RomeroNo ratings yet
- Current Electricity Type 2 PART 1 OF 3 ENG PDFDocument30 pagesCurrent Electricity Type 2 PART 1 OF 3 ENG PDFRafael MadeiraNo ratings yet
- Oise Dissertation GuidelinesDocument6 pagesOise Dissertation GuidelinesPaySomeoneToWriteAPaperCanada100% (1)
- HERMIE ANN COMENDADOR - Hermietot ComendadorDocument4 pagesHERMIE ANN COMENDADOR - Hermietot ComendadorJaromohom AngelaNo ratings yet