You might also like
- Penyakit Katup Jantung-Kuliah DR ErlinaDocument70 pagesPenyakit Katup Jantung-Kuliah DR ErlinaAdhiatma DotNo ratings yet
- Lecture 17a VHDDocument70 pagesLecture 17a VHDKishan ArrumugamNo ratings yet
- Aortic StenosisDocument37 pagesAortic Stenosissarguss14No ratings yet
- 4 Valvular Heart Disease ICMPD (Autosaved)Document30 pages4 Valvular Heart Disease ICMPD (Autosaved)mus zaharaNo ratings yet
- An Overview of Valvular Heart DiseaseDocument42 pagesAn Overview of Valvular Heart DiseaseSantosh NaliathNo ratings yet
- Valvular Heart DiseaseDocument10 pagesValvular Heart DiseaseEzyan SyaminNo ratings yet
- Robbi Zidnii Ilmaa, War Zuqnii Fahmaa, AamiinDocument109 pagesRobbi Zidnii Ilmaa, War Zuqnii Fahmaa, Aamiinfitrian amwaalunNo ratings yet
- 78 - Endocarditis, ValvedzDocument15 pages78 - Endocarditis, ValvedzStefani SihombingNo ratings yet
- UMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiDocument132 pagesUMS20 Medical 20 Short 20 and 20 Long 20 Cases 20 Record 20 Second 20 EditiUchiha AnzarNo ratings yet
- VHDDocument102 pagesVHDPenuhTandaTanyaNo ratings yet
- Valvular Heart Disease: Joko AnggoroDocument53 pagesValvular Heart Disease: Joko AnggoroReza SatriaNo ratings yet
- Nursing Acn-IiDocument80 pagesNursing Acn-IiMunawar100% (6)
- K7 - Penyakit Jantung Katub-ANNDocument38 pagesK7 - Penyakit Jantung Katub-ANNXeniel AlastairNo ratings yet
- Valvular Heart DiseaseDocument41 pagesValvular Heart DiseaseVirendra Shekhawat100% (1)
- Heart Valve DiseaseDocument67 pagesHeart Valve DiseaseSaba SivaNo ratings yet
- Rheumatic Heart DiseaseDocument47 pagesRheumatic Heart DiseaseGideon K. MutaiNo ratings yet
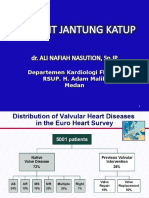
- Valvular Heart Disease: Departemen Kardiologi Dan Kedokteran Vaskular FK UsuDocument38 pagesValvular Heart Disease: Departemen Kardiologi Dan Kedokteran Vaskular FK UsuDumora FatmaNo ratings yet
- Valvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMDocument69 pagesValvular Heart Disease: Presented by DR Mirjana Milutinovic Professor, SJSMAbanoub AwadallaNo ratings yet
- Valvular Heart DiseaseDocument73 pagesValvular Heart Diseaseindia2puppy100% (4)
- Rheumatic Heart DiseaseDocument35 pagesRheumatic Heart DiseaseSAYMABANUNo ratings yet
- PJB Pada Dewasa AASDocument54 pagesPJB Pada Dewasa AAS1e23e2ewNo ratings yet
- Valvular Heart Disease: Bekele T. (MD)Document47 pagesValvular Heart Disease: Bekele T. (MD)alehegn beleteNo ratings yet
- Valvular Heart DiseaseDocument85 pagesValvular Heart DiseaseWilliam Lie100% (2)
- Aortic Stenosis AmendillaDocument31 pagesAortic Stenosis AmendillaVadim BursacovschiNo ratings yet
- Slide Untuk SabtuDocument35 pagesSlide Untuk SabtuAgustinus FatollaNo ratings yet
- Amboss:CardioDocument18 pagesAmboss:CardioNicole Juliette CCNo ratings yet
- Pathophys VHD-Final (Budi S. Pikir)Document155 pagesPathophys VHD-Final (Budi S. Pikir)Muhammad DaviqNo ratings yet
- Mitral Stenosis-RarestDocument9 pagesMitral Stenosis-RarestWen Jie LauNo ratings yet
- Angelina A Joho MSC in Critical Care and TraumaDocument50 pagesAngelina A Joho MSC in Critical Care and TraumaZabron LuhendeNo ratings yet
- Penyakit Jantung KatupDocument35 pagesPenyakit Jantung Katupdwi ariskaNo ratings yet
- Aortic Stenosis - LecturioDocument13 pagesAortic Stenosis - Lecturiokujtimepira2No ratings yet
- Dr. Musnidarti, SPJP, FihaDocument72 pagesDr. Musnidarti, SPJP, FihasovianNo ratings yet
- MRCP Revision NotesDocument41 pagesMRCP Revision NotesMudassar Waseem100% (1)
- Short Cases in Medicine ColomboDocument70 pagesShort Cases in Medicine Colombodileepa madurangaNo ratings yet
- Congenital Heart Disease-2Document57 pagesCongenital Heart Disease-2Deepika LamichhaneNo ratings yet
- InternalDocument29 pagesInternalLuai Tuma KhouryNo ratings yet
- Congenital Heart Disease (CHD) : Kussia Ayano (MD)Document54 pagesCongenital Heart Disease (CHD) : Kussia Ayano (MD)Yemata HailuNo ratings yet
- MS MR As ArDocument21 pagesMS MR As ArTamim IshtiaqueNo ratings yet
- 3 CRHD CMP and CHDDocument73 pages3 CRHD CMP and CHDDammaqsaa W BiyyanaaNo ratings yet
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Document51 pagesDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Jansenkoh MRCP PacesDocument209 pagesJansenkoh MRCP PacesBob Yong83% (6)
- Prof. Iwan - Kuliah RHD and VHD-1Document41 pagesProf. Iwan - Kuliah RHD and VHD-1delia rahmaNo ratings yet
- VHD Inter FinalDocument84 pagesVHD Inter Finalfitrah fajrianiNo ratings yet
- Congenital Heart Diseases: Prof. Dr. Md. Nazrul IslamDocument23 pagesCongenital Heart Diseases: Prof. Dr. Md. Nazrul IslamprajwalNo ratings yet
- Valvular Heart DiseaseDocument5 pagesValvular Heart DiseaseElyas MehdarNo ratings yet
- Aortic StenosisDocument15 pagesAortic StenosisSanjeet SahNo ratings yet
- Tips and Tricks in Management of Patients With CHDDocument46 pagesTips and Tricks in Management of Patients With CHDDrMarcus KeyboardNo ratings yet
- CVS 3-3 PDFDocument24 pagesCVS 3-3 PDFafaq alismailiNo ratings yet
- Congenital Heart DeseasesDocument54 pagesCongenital Heart DeseasesAntony100% (1)
- Pulmonary Valve StenosisDocument6 pagesPulmonary Valve StenosisKobby AmoahNo ratings yet
- Achd Ug OriginalDocument43 pagesAchd Ug OriginalchristyNo ratings yet
- Emergency EchocardiographyDocument62 pagesEmergency Echocardiographyansarijaved100% (1)
- Cardiac SurgeryDocument110 pagesCardiac SurgeryChristopher McAndrew100% (1)
- Mitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeDocument16 pagesMitral Stenosis: Dr. Mohammed Asrafur Rahman MBBS, Bcs (H), MD Resident (Internal Medicine) (P-A) Chattogram Medical CollegeAsrafur RahmanNo ratings yet
- Cctga PcicsDocument9 pagesCctga PcicsAdrian KhomanNo ratings yet
- Top Ten (Or 11) EKG KillersDocument84 pagesTop Ten (Or 11) EKG Killersphausknecht100% (1)
- DR Abdulkareem Al Othman Valvular HDDocument10 pagesDR Abdulkareem Al Othman Valvular HDDarawan MirzaNo ratings yet
- Pneumonia: Dr. Tjatur Winarsanto SPPDDocument46 pagesPneumonia: Dr. Tjatur Winarsanto SPPDanisamayaNo ratings yet
- Appendicitis - PeritonitisDocument37 pagesAppendicitis - PeritonitisanisamayaNo ratings yet
- Kuliah Batu RevisiDocument23 pagesKuliah Batu RevisianisamayaNo ratings yet
- Kuliah Penis & Scrotum RevisiDocument13 pagesKuliah Penis & Scrotum Revisianisamaya0% (1)
- CasriDocument1 pageCasrianisamayaNo ratings yet
- LukmanDocument1 pageLukmananisamayaNo ratings yet
- Ahmad SururiDocument1 pageAhmad SururianisamayaNo ratings yet
- LukmanDocument1 pageLukmananisamayaNo ratings yet
- Mitral Valve ReplacementDocument44 pagesMitral Valve ReplacementYusardi R Pradana100% (1)
- Valve Repair & ReplacementDocument27 pagesValve Repair & ReplacementmaibejoseNo ratings yet
- Cvs - Clinical NotesDocument38 pagesCvs - Clinical NotessekaralingamNo ratings yet
- Fitz Cardiology Paces NotesDocument26 pagesFitz Cardiology Paces NotesMuhammad BilalNo ratings yet
- Mods of UltrasoundDocument22 pagesMods of UltrasoundEnrique Valdez JordanNo ratings yet
- Aortic Root Surgery PDFDocument618 pagesAortic Root Surgery PDFVikas Kumar KeshriNo ratings yet
- Congenital Heart Disease in CatsDocument5 pagesCongenital Heart Disease in Catsmatias66No ratings yet
- Chronic Mitral Regurgitation and Aortic Regurgitation: Have Indications For Surgery Changed?Document9 pagesChronic Mitral Regurgitation and Aortic Regurgitation: Have Indications For Surgery Changed?mamuyaNo ratings yet
- Cardiovascular SystemDocument26 pagesCardiovascular SystemRismawatiNo ratings yet
- Diastolic Heart Failure AssessmentDocument16 pagesDiastolic Heart Failure AssessmentMd. ashfaque Ahemmed khanNo ratings yet
- Design and Finite Element-Based Fatigue Prediction of A New Self-Expandable Percutaneous Mitral Valve StentDocument6 pagesDesign and Finite Element-Based Fatigue Prediction of A New Self-Expandable Percutaneous Mitral Valve StenthanNo ratings yet
- Rheumatic Fever and Rheumatic Heart DiseaseDocument54 pagesRheumatic Fever and Rheumatic Heart DiseaseFian AldyNo ratings yet
- Chapter 31: Structure and Function of The Cardiovascular and Lymphatic SystemsDocument12 pagesChapter 31: Structure and Function of The Cardiovascular and Lymphatic SystemsMelissa WrightNo ratings yet
- B.inggris KtiDocument61 pagesB.inggris KtiDimasNo ratings yet
- Case Stenosis Aorta + RegurgitationDocument58 pagesCase Stenosis Aorta + RegurgitationRuth Faustine Jontah RayoNo ratings yet
- Vena Contracta Width Is A Semi-Quantitative Parameter To Assess The Severity of Mitral RegurgitationDocument20 pagesVena Contracta Width Is A Semi-Quantitative Parameter To Assess The Severity of Mitral Regurgitationalex leeNo ratings yet
- Cvs MCQ Exam 2008Document14 pagesCvs MCQ Exam 2008ZH. omg sarNo ratings yet
- PericarditisDocument120 pagesPericarditis18sn02nr059No ratings yet
- Basic ECG Interpretation 2 0 E Learning Notebook PDFDocument164 pagesBasic ECG Interpretation 2 0 E Learning Notebook PDFRoe Briones100% (1)
- 04 Mediastinum, HeartDocument27 pages04 Mediastinum, HeartShaira Aquino VerzosaNo ratings yet
- Pathology (Awasir)Document152 pagesPathology (Awasir)Yousef TaqatqehNo ratings yet
- Dr.C.N.manjunath The Eminent CardiologistDocument19 pagesDr.C.N.manjunath The Eminent Cardiologistacharla5549100% (1)
- CT and MR in Cardiology 1St Edition Suhny Abbara Full ChapterDocument67 pagesCT and MR in Cardiology 1St Edition Suhny Abbara Full Chapterelizabeth.dew603100% (8)
- FRACP Written Exam Otago MCQ Book 2016Document470 pagesFRACP Written Exam Otago MCQ Book 2016Qiliang Liu100% (2)
- CVS. Questions and AnswersDocument6 pagesCVS. Questions and AnswersOmar HNo ratings yet
- Anaesthesia in Dogs and Cats With Cardiac DiseaseDocument19 pagesAnaesthesia in Dogs and Cats With Cardiac DiseaseALEJANDRA MADRIGALNo ratings yet
- Heart Valve Disease Treatment Guide - Cleveland ClinicDocument12 pagesHeart Valve Disease Treatment Guide - Cleveland ClinicGuillermo CenturionNo ratings yet
- POCUS ProceduresDocument123 pagesPOCUS Proceduresjaimin 666100% (1)
- Block 1 Board Review - Lecture NotesDocument127 pagesBlock 1 Board Review - Lecture NotesCece RereNo ratings yet
- 1700 Subject Wise by PLAB Zillas (Bookmarked)Document380 pages1700 Subject Wise by PLAB Zillas (Bookmarked)hackchild100% (1)