You might also like
- ADHF Responsi Abduh Saskia KevinDocument26 pagesADHF Responsi Abduh Saskia KevinarsyaNo ratings yet
- MR Paru 150116 TwaDocument18 pagesMR Paru 150116 Twaadelia putri wirandaniNo ratings yet
- Preskas Acs FinalDocument45 pagesPreskas Acs FinalIlham NoeryosanNo ratings yet
- Asuhan Keperawatan Gawat Darurat TN.H IcuDocument9 pagesAsuhan Keperawatan Gawat Darurat TN.H IcuDwy RizqiNo ratings yet
- Laporan Jaga 13JULIDocument24 pagesLaporan Jaga 13JULIDefriyan RamziNo ratings yet
- MR 29-08-22Document17 pagesMR 29-08-22syahda nabillaNo ratings yet
- CBD AF Pada Impending Thyroid Storm IMA DR - VYADocument27 pagesCBD AF Pada Impending Thyroid Storm IMA DR - VYAAfrilia IntanNo ratings yet
- Anestesi Spinal Pada TURP Dengan Penyulit HipertensiDocument56 pagesAnestesi Spinal Pada TURP Dengan Penyulit HipertensiJason SutandarNo ratings yet
- Syok KardiogenikDocument19 pagesSyok KardiogenikIrma Pryuni AinandaNo ratings yet
- Morning Report RochaetiDocument57 pagesMorning Report RochaetirashbahatNo ratings yet
- Yovita 31 JanuariDocument42 pagesYovita 31 JanuariKiyo RaNo ratings yet
- Laporan Kasus Stemi AnissaDocument14 pagesLaporan Kasus Stemi AnissaAndriNo ratings yet
- CRS - Enita - Stemi AnteriorDocument38 pagesCRS - Enita - Stemi AnteriorLiana Ika SuwandyNo ratings yet
- Laporan Kasus StemiDocument14 pagesLaporan Kasus StemiAnonymous GUP54qEONo ratings yet
- Copy-LAPORAN JAGA 21.10.2022 MO BK MTDocument12 pagesCopy-LAPORAN JAGA 21.10.2022 MO BK MTbikoadjisukmorahardjoNo ratings yet
- Debridement Fournier GangrenDocument49 pagesDebridement Fournier GangrenPrimidia SusantiNo ratings yet
- Lapsus EmdDocument20 pagesLapsus EmdPubdok InternaNo ratings yet
- PB Per Tanggal 7 Nov 23Document6 pagesPB Per Tanggal 7 Nov 23masitha yusmarNo ratings yet
- Case Report Bedah BTKV FrcosDocument8 pagesCase Report Bedah BTKV FrcosAnonymous h0DxuJTNo ratings yet
- Laporan Kasus STEMIDocument52 pagesLaporan Kasus STEMIharisabdurNo ratings yet
- VT Dengan NadiDocument19 pagesVT Dengan NadiSeptian SoegiartoNo ratings yet
- Borang RSMB InesDocument179 pagesBorang RSMB InesSofia SalsabilaNo ratings yet
- NSTEMIDocument19 pagesNSTEMIIswahyudi SenoNo ratings yet
- WelehwelehDocument55 pagesWelehwelehSovian Anugrah Lumban GaolNo ratings yet
- Case Report JantungDocument18 pagesCase Report JantungFerrina UfianiNo ratings yet
- Lapkas CHF Marelan DR Gin FixDocument31 pagesLapkas CHF Marelan DR Gin FixAndreas SiagianNo ratings yet
- Lapkas - NonIlmiah - Fajriati Samsi A.Tadda - Demam TypoidDocument26 pagesLapkas - NonIlmiah - Fajriati Samsi A.Tadda - Demam TypoidBambang Triwahyudi Abdul HadiNo ratings yet
- LAPORAN KASUS Tn. DEDI PURWADIDocument5 pagesLAPORAN KASUS Tn. DEDI PURWADIditraNo ratings yet
- Kasus Stase IpdDocument61 pagesKasus Stase IpdRadityaRezhaNo ratings yet
- Pengkajian OrlandoDocument5 pagesPengkajian Orlandoyovanimanuel imanuelNo ratings yet
- Case Report ACSDocument50 pagesCase Report ACSastridya nabilahNo ratings yet
- Tn. P - 69 THN - GEA + Dehidrasi Ringan +vomiting + Susp AKI - IGD - InternaDocument15 pagesTn. P - 69 THN - GEA + Dehidrasi Ringan +vomiting + Susp AKI - IGD - Internatom jerryNo ratings yet
- CHF Kasus KecilDocument17 pagesCHF Kasus KecilFlorensia WodaNo ratings yet
- Bismillah em Krisis Hiperglikemia P1Document45 pagesBismillah em Krisis Hiperglikemia P1mariskaNo ratings yet
- CBD Kardio-Interna - Giovani Christin F PurbaDocument29 pagesCBD Kardio-Interna - Giovani Christin F PurbaAnonymous xv9UDvKLNo ratings yet
- Diky RamlanDocument10 pagesDiky RamlanRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Case 2Document22 pagesCase 2Febrina HafidaNo ratings yet
- Laporan Kasus KetoasidosisDocument75 pagesLaporan Kasus KetoasidosisAnandaNo ratings yet
- CASE REPORT Pasien ConfDocument8 pagesCASE REPORT Pasien Confseruni medinaNo ratings yet
- 6456 - Refkas GA Dengan ET Pada VP ShuntDocument77 pages6456 - Refkas GA Dengan ET Pada VP ShuntferonicaNo ratings yet
- LAPORAN KASUS STEMI INFERIOR + TAVB + DM Tipe 2Document41 pagesLAPORAN KASUS STEMI INFERIOR + TAVB + DM Tipe 2JunarNo ratings yet
- CKD STAGE V ON HD, ANEMIA RENAL, HIPERTENSI GRADE II, ASIDOSIS METABOLIK, EDEMA PARU DD PNEUMONIA COVID 19Document24 pagesCKD STAGE V ON HD, ANEMIA RENAL, HIPERTENSI GRADE II, ASIDOSIS METABOLIK, EDEMA PARU DD PNEUMONIA COVID 19Nadilla De PutriNo ratings yet
- Kad & StemiDocument21 pagesKad & Steminurul ilmiaNo ratings yet
- 17-6-2022 Ny. Ovince Hau - Dr. Agus, SP - Og - KETDocument22 pages17-6-2022 Ny. Ovince Hau - Dr. Agus, SP - Og - KETukmppd undanaNo ratings yet
- Laporan Kasus, Refleksi Kasus, Tutorial Klinik Cardio - Pradnya Paramita - 2171121027Document27 pagesLaporan Kasus, Refleksi Kasus, Tutorial Klinik Cardio - Pradnya Paramita - 2171121027Ayu Putri DharmaNo ratings yet
- LAPKAS Nyeri DadaDocument18 pagesLAPKAS Nyeri DadaBimaTarunaSaktiNo ratings yet
- Laporan Kasus ClaviculaDocument7 pagesLaporan Kasus ClaviculaakbarNo ratings yet
- Presentasi Kasus 1: Supraventrikular Takikardi: Mutia Aridha Imannisa, DRDocument32 pagesPresentasi Kasus 1: Supraventrikular Takikardi: Mutia Aridha Imannisa, DRNinisNo ratings yet
- Resume 1Document14 pagesResume 1nilaNo ratings yet
- Responsi Paru CopdDocument46 pagesResponsi Paru Copdbibon27No ratings yet
- Mini Cex 4 DR ChandraminDocument22 pagesMini Cex 4 DR Chandraminmanar siti denariNo ratings yet
- Apache 2Document28 pagesApache 2Hannisa Rizki RiansyahNo ratings yet
- Annisa Illona A - Presentasi KasusDocument34 pagesAnnisa Illona A - Presentasi Kasusannisa illonaNo ratings yet
- MR Jaga 11 AprilDocument15 pagesMR Jaga 11 Aprildimas oktoferryNo ratings yet
- LAPSUS Atrial FibrilasiDocument41 pagesLAPSUS Atrial FibrilasiAllia SalsabilaNo ratings yet
- Presentation HipertiroidDocument42 pagesPresentation HipertiroidBalrajk DhillonNo ratings yet
- Lapsus StemiDocument10 pagesLapsus StemiUmmu AimanNo ratings yet
- Case NitaDocument31 pagesCase NitaMuhammad Noer Gusti AnggaraNo ratings yet
- Asesmen Awal Pasien Korban Kekerasan Dan TerlantarDocument2 pagesAsesmen Awal Pasien Korban Kekerasan Dan TerlantarNur ArafahNo ratings yet
- 1.3 Dr. Priyo - Analisis Karakter Virus SARS-COV2 - Medtrain2020 FKUApdf PDFDocument31 pages1.3 Dr. Priyo - Analisis Karakter Virus SARS-COV2 - Medtrain2020 FKUApdf PDFNur ArafahNo ratings yet
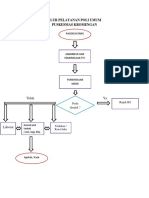
- Alur Pelayanan Poli Umum Dan SopDocument2 pagesAlur Pelayanan Poli Umum Dan SopNur ArafahNo ratings yet
- BAB III Peta Konsep TBDocument3 pagesBAB III Peta Konsep TBNur ArafahNo ratings yet
- Cara Membuat KhotbahDocument10 pagesCara Membuat KhotbahNur ArafahNo ratings yet
- Penyuluhan Cuci TanganDocument11 pagesPenyuluhan Cuci TanganNur ArafahNo ratings yet
- Pelayanan MedisDocument37 pagesPelayanan MedisNur ArafahNo ratings yet
- Lamp-4 - Bahan Ajar Urbanisasi (Pita Giri)Document26 pagesLamp-4 - Bahan Ajar Urbanisasi (Pita Giri)Nur ArafahNo ratings yet