You might also like
- HeadacheDocument36 pagesHeadacheabenezer g/kirstosNo ratings yet
- Cooh Cooh NH OH: Tryptophan 5-HydroxytryptophanDocument14 pagesCooh Cooh NH OH: Tryptophan 5-HydroxytryptophankoushiksarkerNo ratings yet
- Unit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIDocument38 pagesUnit 2 Anti Migraine and Drugs For Trigeminal Neuralgia Pharmacy-IIAsad MirajNo ratings yet
- Myasthenia GravisDocument2 pagesMyasthenia GravisMarissa AsimNo ratings yet
- Toxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiDocument59 pagesToxicology: by Group 4 2018/2019 Tan Geok Eng Reena DewiTan Geok EngNo ratings yet
- Therapy of Migraine: An Overview: By-Parul Dixit Iind Trimester, M.Pharm (Pharmacology), SPTM, NmimsDocument29 pagesTherapy of Migraine: An Overview: By-Parul Dixit Iind Trimester, M.Pharm (Pharmacology), SPTM, NmimsParul DixitNo ratings yet
- 4 HeadacheDocument33 pages4 HeadacheNathaniel BudayNo ratings yet
- A MigraineDocument32 pagesA MigraineA A D H INo ratings yet
- Anti MigraineDocument32 pagesAnti MigraineIzzat NazmiNo ratings yet
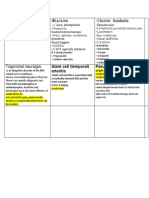
- Tension Headache Migraine - Cluster Headache: Giant Cell (Temporal) Arteritis Pseudotumor CerebriDocument1 pageTension Headache Migraine - Cluster Headache: Giant Cell (Temporal) Arteritis Pseudotumor CerebrifathiNo ratings yet
- CNS DrugsDocument57 pagesCNS DrugsHussein Al-jmrawiNo ratings yet
- Null 1Document60 pagesNull 1tbuyinza21apNo ratings yet
- Epilepsy Class - DrdhritiDocument81 pagesEpilepsy Class - DrdhritidbrahmaNo ratings yet
- NPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesDocument83 pagesNPLEX Combination Review Neurology - A: Paul S. Anderson, ND Medical Board Review ServicesValeria AcevedoNo ratings yet
- Yuli - Kuliah Blok 11 - Headache 2019Document66 pagesYuli - Kuliah Blok 11 - Headache 2019reshaNo ratings yet
- PsychopharmacologyDocument98 pagesPsychopharmacologyMontero, Ma. Cecilia - BSN 3-B100% (1)
- Drugs For Treatment of Migraine and Vertigo: Dharma Permana, Apt, PHDDocument27 pagesDrugs For Treatment of Migraine and Vertigo: Dharma Permana, Apt, PHDZera DirgantaraNo ratings yet
- Drugs Acting On The Nervous SystemDocument123 pagesDrugs Acting On The Nervous SystemIretiola AdeleruNo ratings yet
- Drugs Acting On The Nervous SystemDocument123 pagesDrugs Acting On The Nervous SystemIretiola Adeleru100% (1)
- CNS StimulantsDocument26 pagesCNS StimulantsShivaNo ratings yet
- Drug StudyDocument11 pagesDrug StudyJohn LesterNo ratings yet
- Anti ConvulsantDocument42 pagesAnti ConvulsantAkmal SafwanNo ratings yet
- Top DrugsDocument12 pagesTop DrugsStephanie Villanueva AdvinculaNo ratings yet
- Anti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCDocument17 pagesAnti-Depressant Drugs: Presented by L.Nithish Shankar Ii Year Mbbs KGMCÑiťhišh Śhankąŕ LóganáthánNo ratings yet
- Drugs Used in Mental IllnessDocument60 pagesDrugs Used in Mental IllnessDixa MeNo ratings yet
- Module 10Document5 pagesModule 10Yuki Xairah TunayNo ratings yet
- TOP DRUGS - Doc Version 1Document12 pagesTOP DRUGS - Doc Version 1Charme Jean RaygonNo ratings yet
- I Co Glaucoma GuidelinesDocument15 pagesI Co Glaucoma GuidelinesRizqan Fahlevvi AkbarNo ratings yet
- Pharmacotherapy of Migraine: DR Manukumar Post Graduate Dept of Pharmacology VMMC & Safdarjung HospitalDocument49 pagesPharmacotherapy of Migraine: DR Manukumar Post Graduate Dept of Pharmacology VMMC & Safdarjung HospitalshravaniNo ratings yet
- Antiepileptic DrugsDocument63 pagesAntiepileptic Drugsvpd100% (1)
- Insomnia - Conceptualization and Management in 2009Document40 pagesInsomnia - Conceptualization and Management in 2009Georgy PanchenkoNo ratings yet
- NEUROPHARMACOLOGYDocument36 pagesNEUROPHARMACOLOGYDebika DasNo ratings yet
- PsychopharmacologyDocument50 pagesPsychopharmacologyapi-3703352No ratings yet
- Conscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantDocument84 pagesConscious Sedation: Hayel Gharaibeh, MD. Anesthesia ConsultantKhaled GharaibehNo ratings yet
- CNS StimulantsDocument89 pagesCNS StimulantsMwanja Moses100% (1)
- CNS PharmaDocument10 pagesCNS Pharmaahmedhelper300No ratings yet
- Headache:: A Practical ApproachDocument93 pagesHeadache:: A Practical ApproachSadiaNo ratings yet
- Drugs Used in The Treatment of Pain and Affecting The Musculoskeletal SystemDocument34 pagesDrugs Used in The Treatment of Pain and Affecting The Musculoskeletal SystemAnna Lin YeeNo ratings yet
- PsychopharmacologyDocument50 pagesPsychopharmacology4dsb6ctx67No ratings yet
- Seizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HDocument70 pagesSeizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HRohini RaiNo ratings yet
- Anti-Depressants: Soumya Mary 1 Year MSC (N)Document22 pagesAnti-Depressants: Soumya Mary 1 Year MSC (N)Salman HabeebNo ratings yet
- Pharmacology: Drugs That Affect The: Nervous SystemDocument84 pagesPharmacology: Drugs That Affect The: Nervous SystemSameh Saber100% (1)
- Barbiturate Benzodiazepine PoisoningDocument23 pagesBarbiturate Benzodiazepine PoisoningRoman MamunNo ratings yet
- Central Nervous System Agents: Carmencita R. Pacis PHD, ManDocument52 pagesCentral Nervous System Agents: Carmencita R. Pacis PHD, ManTWINNY JOSSANNE CHEERISHANE MINIONNo ratings yet
- Autonomic 1 OkDocument56 pagesAutonomic 1 Okufcwwe133No ratings yet
- Antiseizure AgentsDocument62 pagesAntiseizure Agentsakoeljames8543No ratings yet
- SDL 21 Headaches BMS16091064Document8 pagesSDL 21 Headaches BMS16091064Jonathan YeohNo ratings yet
- Amh Summary 2019 İn One FileDocument220 pagesAmh Summary 2019 İn One FileTatenda BrunoNo ratings yet
- Farmakologi Dari Obat EpilepsiDocument82 pagesFarmakologi Dari Obat EpilepsiDion SaputraNo ratings yet
- Unraveling Migraines: Yousef Elyaman, MD, IfmcDocument56 pagesUnraveling Migraines: Yousef Elyaman, MD, IfmcBerny VillavicencioNo ratings yet
- Psychotropic Drugs: By: Rheajane Aguilar-RosalesDocument77 pagesPsychotropic Drugs: By: Rheajane Aguilar-Rosalesjean samson100% (1)
- F.R 1.3 Farmakologi Obat Antipiretik Dan Induksi DemamDocument64 pagesF.R 1.3 Farmakologi Obat Antipiretik Dan Induksi Demamasa0411 behiraNo ratings yet
- Epileptic Drugs by DR DinaDocument39 pagesEpileptic Drugs by DR DinaseraNo ratings yet
- 8 Cns StimulantsDocument46 pages8 Cns StimulantslouradelNo ratings yet
- AntideprresentDocument54 pagesAntideprresentHadiqa KhanNo ratings yet
- Central Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsDocument33 pagesCentral Nervous System (CNS) Pharmacology (PCL 401) Antiepileptic/Anticonvulsants DrugsJoseph JohnNo ratings yet
- Antiseizure Drugs: By: Aim D. QuttenehDocument9 pagesAntiseizure Drugs: By: Aim D. QuttenehrimNo ratings yet
- Headache & Migraine DrugsDocument59 pagesHeadache & Migraine Drugsjoshua katunziNo ratings yet
- Trigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesFrom EverandTrigeminal Neuralgia: A Beginner's 3-Step Quick Start Guide to Managing TB Through Diet, With Sample RecipesNo ratings yet
- Toksisitas Alkohol Dan Penanganannya PDFDocument9 pagesToksisitas Alkohol Dan Penanganannya PDFvivi novitaliaNo ratings yet
- Toksisitas Alkohol Dan Penanganannya PDFDocument9 pagesToksisitas Alkohol Dan Penanganannya PDFvivi novitaliaNo ratings yet
- Clean Room PharmaDocument39 pagesClean Room PharmadurbcomsonoNo ratings yet
- 28Document7 pages28vivi novitaliaNo ratings yet
- Ota Go 117060Document43 pagesOta Go 117060vivi novitaliaNo ratings yet
- Antibiotic GuidelineDocument116 pagesAntibiotic GuidelineD'nollas LadysNo ratings yet
- Manajemen Publik 2 PDFDocument8 pagesManajemen Publik 2 PDFvivi novitaliaNo ratings yet
- Ota Go 117060Document43 pagesOta Go 117060vivi novitaliaNo ratings yet
- Isdn PMDocument11 pagesIsdn PMPrasdian Nur ChoiriNo ratings yet
- PharmD Handbook14 15 Final LowDocument56 pagesPharmD Handbook14 15 Final Lowvivi novitaliaNo ratings yet
- Clinical Pharma 2Document156 pagesClinical Pharma 2RebwarNo ratings yet
- Form Standarisasi BMHP RSU Jampang Kulon 2020Document6 pagesForm Standarisasi BMHP RSU Jampang Kulon 2020Avrilia Fuji AstutiNo ratings yet
- 2016 Sep RECALLDocument49 pages2016 Sep RECALLkyahuaNo ratings yet
- Burn Management by Tajuu Seid: Surgical WardDocument33 pagesBurn Management by Tajuu Seid: Surgical Wardelias adugnaNo ratings yet
- OB - Normal Labor and DeliveryDocument51 pagesOB - Normal Labor and DeliveryJosh Matthew Rosales33% (3)
- Ternian HCIS InteractiveDocument10 pagesTernian HCIS InteractivetrninsgrpNo ratings yet
- Long-Term Evaluation of Periodontal TherapyDocument16 pagesLong-Term Evaluation of Periodontal TherapyRanuch TakNo ratings yet
- Epidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmDocument5 pagesEpidemiology, Risk Factors, Pathogenesis, and Natural History of Thoracic Aortic AneurysmNathaliazuosNo ratings yet
- User Manual Buble Cpap PDFDocument7 pagesUser Manual Buble Cpap PDFmamahosieleNo ratings yet
- Mna Mini English PDFDocument1 pageMna Mini English PDFLastry WardaniNo ratings yet
- Artificial or Supplimentary FoodDocument4 pagesArtificial or Supplimentary FoodArchana Sahu100% (1)
- ANC ModuleDocument103 pagesANC ModulePreeti ChouhanNo ratings yet
- Letting Go by Atul GawandeDocument18 pagesLetting Go by Atul Gawandetakoyakilovers100% (2)
- IsoketDocument2 pagesIsoketJaessa FelicianoNo ratings yet
- Ficha Tecnica ANTIGENO 120006841 v3 Panbio COVID-19 Ag Nasopharyngeal IFU BoDocument132 pagesFicha Tecnica ANTIGENO 120006841 v3 Panbio COVID-19 Ag Nasopharyngeal IFU BoYessica Marisol Custodio ReinosoNo ratings yet
- UNIT-I: General Pharmacology As Per Syllabus Unit-1, Chapter A (Half)Document18 pagesUNIT-I: General Pharmacology As Per Syllabus Unit-1, Chapter A (Half)Atthapu ThirupathaiahNo ratings yet
- A Guide For G6PDDocument4 pagesA Guide For G6PDshimeath delrosarioNo ratings yet
- HEPATOMEGALY CaseDocument5 pagesHEPATOMEGALY CaseKanwaljeet SinghNo ratings yet
- Pharmacology of The GIT System: CIC Ragasa, RN-MDDocument70 pagesPharmacology of The GIT System: CIC Ragasa, RN-MDCarmencita Ileen Ragasa - AhmedNo ratings yet
- Anti Diare SGDocument17 pagesAnti Diare SGludoy03No ratings yet
- Complete Medical TermsDocument32 pagesComplete Medical TermsSharifa Darayan100% (1)
- Post Insertion Complaints in Complete Dentures - A Never Ending SagaDocument8 pagesPost Insertion Complaints in Complete Dentures - A Never Ending SagaKrupali JainNo ratings yet
- Arrhythmia A ADocument42 pagesArrhythmia A AMohd Faizal KasnanNo ratings yet
- Dental Management of The Patient With HIVAIDS 2002Document6 pagesDental Management of The Patient With HIVAIDS 2002drkameshNo ratings yet
- CLICO Group Health and Life Coverage 1Document12 pagesCLICO Group Health and Life Coverage 1buckianNo ratings yet
- Filosofi Kesehatan MasyarakatDocument4 pagesFilosofi Kesehatan MasyarakatJennilynn YusameNo ratings yet
- FCEM (SA) Part II Past Papers - 2012 Sept 22-1-2014Document7 pagesFCEM (SA) Part II Past Papers - 2012 Sept 22-1-2014matentenNo ratings yet
- Chapter 1: Introduction To Psychiatric NursingDocument5 pagesChapter 1: Introduction To Psychiatric NursingWarrenPeaceNo ratings yet
- Abilify Dosing GuideDocument2 pagesAbilify Dosing GuidemtassyNo ratings yet
- SAS 14 MCNDocument2 pagesSAS 14 MCNKristinelou Marie N. Reyna0% (1)