You might also like
- Health Care Professionals 2015Document26 pagesHealth Care Professionals 2015MACON824No ratings yet
- Unintentional Injury 2015Document40 pagesUnintentional Injury 2015MACON824No ratings yet
- Hta 2015Document26 pagesHta 2015MACON824No ratings yet
- Thyroid Gland PDFDocument47 pagesThyroid Gland PDFMACON824No ratings yet
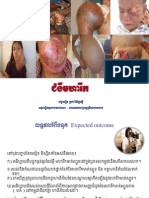
- Cmgwmharik: Evc Bnðit R) Ak Bisidærgsi Gnubnðitsuxpabsafarn - ÉketsgaharubtßmönigrbbgaharDocument39 pagesCmgwmharik: Evc Bnðit R) Ak Bisidærgsi Gnubnðitsuxpabsafarn - ÉketsgaharubtßmönigrbbgaharMACON824No ratings yet
- Le DipylidiumcaninumDocument3 pagesLe DipylidiumcaninumMACON824No ratings yet
- Chapter 24 Urinary BladderDocument42 pagesChapter 24 Urinary BladderMACON824No ratings yet
- Chapter 28 Pelvis and Perineum PDFDocument89 pagesChapter 28 Pelvis and Perineum PDFMACON824No ratings yet
- Chapter 29 Lymphatic System PDFDocument24 pagesChapter 29 Lymphatic System PDFMACON824No ratings yet
- Chapter 26 Female Genital SystemDocument79 pagesChapter 26 Female Genital SystemMACON824No ratings yet
- Chapter 26 Female Genital SystemDocument79 pagesChapter 26 Female Genital SystemMACON824No ratings yet
- Chapter 12 Great Vessels in The AbdomenDocument36 pagesChapter 12 Great Vessels in The AbdomenMACON824No ratings yet
- Chapter 20 Extrahepatic Biliary Tract and Gall BladderDocument63 pagesChapter 20 Extrahepatic Biliary Tract and Gall BladderMACON824No ratings yet
- Chapter 22 SpleenDocument69 pagesChapter 22 SpleenMACON824100% (1)
- Chapter 23 Kidneys and UretersDocument71 pagesChapter 23 Kidneys and UretersMACON824No ratings yet
- Chapter 21 PancreasDocument102 pagesChapter 21 PancreasMACON824No ratings yet
- Chapter 14 EsophagusDocument48 pagesChapter 14 EsophagusSMEY204No ratings yet
- Chapter 15 StomachDocument129 pagesChapter 15 StomachMACON824No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Orientation in PIMAMDocument63 pagesOrientation in PIMAMEunicee ElardoNo ratings yet
- Mental RetardationDocument19 pagesMental RetardationGuna gamNo ratings yet
- Source E Learning NCM 121Document11 pagesSource E Learning NCM 121Nathaniel PulidoNo ratings yet
- Respiratory ExaminationDocument19 pagesRespiratory ExaminationMohini33% (3)
- Treatment For Aplastic AnemiaDocument13 pagesTreatment For Aplastic Anemiagustianto hutama pNo ratings yet
- Otc-Eth 17 Mei 23Document17 pagesOtc-Eth 17 Mei 23testy dwi sNo ratings yet
- EKG Cheat Sheet - Henry Del RosarioDocument1 pageEKG Cheat Sheet - Henry Del RosarioanwarNo ratings yet
- Comprehensive Nursing Care in Transplant Unit-1-1Document47 pagesComprehensive Nursing Care in Transplant Unit-1-1Rajani Singh BaghelNo ratings yet
- Awareness and Acceptance of Covid-19 Vaccines Among Non-Medical Students - A Cross Sectional StudyDocument29 pagesAwareness and Acceptance of Covid-19 Vaccines Among Non-Medical Students - A Cross Sectional StudyJohn Cyprian AbeloNo ratings yet
- Types of AnesthesiaDocument1 pageTypes of AnesthesiaImran PinjariNo ratings yet
- Three Years of H CL TherapyDocument50 pagesThree Years of H CL TherapyVíctor ValdezNo ratings yet
- Transposition of The Great ArteriesDocument118 pagesTransposition of The Great ArteriesJoan Rae Tan100% (1)
- Andreas Roth, Orthopedic and Trauma Findings - Examination Techniques, Clinical Evaluation, Clinical Presentation (2017)Document224 pagesAndreas Roth, Orthopedic and Trauma Findings - Examination Techniques, Clinical Evaluation, Clinical Presentation (2017)Mariana Carneiro100% (2)
- High Condylectomy For The Treatment of Mandibular Condylar Hyperplasia: A Systematic Review of The LiteratureDocument12 pagesHigh Condylectomy For The Treatment of Mandibular Condylar Hyperplasia: A Systematic Review of The Literaturemarcela0426No ratings yet
- SMS Result and Data 2021Document161 pagesSMS Result and Data 2021ChinaNo ratings yet
- Hb301 MicrocuvettesDocument48 pagesHb301 MicrocuvettesTrung LeNo ratings yet
- 06 Clinical Pathology MCQs With Answers 1Document29 pages06 Clinical Pathology MCQs With Answers 1Habib Ullah100% (1)
- Dry Eye Syndrome - Diagnosis and Management: Dr. Jeffrey CF PONGDocument3 pagesDry Eye Syndrome - Diagnosis and Management: Dr. Jeffrey CF PONGVeronica Yosita AnandaNo ratings yet
- John Henry O. Valencia: Signature Over Printed Name Director of Nursing Service (Signature Over Printed Name)Document2 pagesJohn Henry O. Valencia: Signature Over Printed Name Director of Nursing Service (Signature Over Printed Name)John Henry ValenciaNo ratings yet
- Neurological Disorders: Prof. Bernardo Fernandez IIDocument33 pagesNeurological Disorders: Prof. Bernardo Fernandez IIBernardNo ratings yet
- IM EAMC ENDORSEMENT (Updated Feb 2020)Document7 pagesIM EAMC ENDORSEMENT (Updated Feb 2020)Joshua Elijah ArsenioNo ratings yet
- TCP gw3 - 2Document99 pagesTCP gw3 - 2Krizel Clare San FelipeNo ratings yet
- Sawai, 2014Document8 pagesSawai, 2014Suci CahyaniNo ratings yet
- Watery Eye: Magdy Fawzy $ Taha Sarhan Prof of OphthalmologyDocument93 pagesWatery Eye: Magdy Fawzy $ Taha Sarhan Prof of OphthalmologymiemednoteNo ratings yet
- Learn To PredictDocument1 pageLearn To PredictKelley WalkerNo ratings yet
- Endodontic Periapical Lesion - An Overview On The Etiology, Diagnosis and Current Treatment ModalitiesDocument14 pagesEndodontic Periapical Lesion - An Overview On The Etiology, Diagnosis and Current Treatment ModalitiesGurudutt NayakNo ratings yet
- Tooth Decay and Highly Conservative TreatmentsDocument26 pagesTooth Decay and Highly Conservative TreatmentsJose Ignacio ZalbaNo ratings yet
- Name - Period - AP Biology Date - Raven Chapter 44 Guided Notes: Circulation & Respiration CirculationDocument8 pagesName - Period - AP Biology Date - Raven Chapter 44 Guided Notes: Circulation & Respiration CirculationDBQNo ratings yet
- Health Issues in The PhilippinesDocument2 pagesHealth Issues in The PhilippinesHisoka MorowNo ratings yet
- Información: Estado Tipo de Participantes Rangos de EdadDocument11 pagesInformación: Estado Tipo de Participantes Rangos de EdadAlondraNo ratings yet