You might also like
- Agreement For Providing Security ServicesDocument6 pagesAgreement For Providing Security ServicesSridhara babu. N - ಶ್ರೀಧರ ಬಾಬು. ಎನ್94% (16)
- End of The AffairDocument8 pagesEnd of The AffairThea MonjeNo ratings yet
- Atlas of Trauma: Operative Techniques, Complications and ManagementFrom EverandAtlas of Trauma: Operative Techniques, Complications and ManagementPaula FerradaNo ratings yet
- CMO 9, S. 2008 - Approved - PS For BSMEDocument17 pagesCMO 9, S. 2008 - Approved - PS For BSMEzakibrant23100% (1)
- Power Point Postural DrainageDocument32 pagesPower Point Postural DrainageTabby Mendence100% (1)
- Prudential Bank Vs IACDocument1 pagePrudential Bank Vs IACYohanna J K GarcesNo ratings yet
- Proposed Water Tank Design A Solution To North Poblacion San Fernandos Inadequate Water SupplyDocument126 pagesProposed Water Tank Design A Solution To North Poblacion San Fernandos Inadequate Water SupplyZynne Chlyden ParinoNo ratings yet
- Bce 222 Tos Exam - 1Document1 pageBce 222 Tos Exam - 1Michelle DaarolNo ratings yet
- PIA B2 - Module 2 (PHYSICS) SubModule 2.3 (Thermodynamics) FinalDocument32 pagesPIA B2 - Module 2 (PHYSICS) SubModule 2.3 (Thermodynamics) Finalsamarrana1234679No ratings yet
- Acute Inhalation InjuryDocument9 pagesAcute Inhalation InjuryahmadNo ratings yet
- GEN PHYSICS 1 MODULE (Midterm and Finals)Document49 pagesGEN PHYSICS 1 MODULE (Midterm and Finals)Crisanta GanadoNo ratings yet
- Chronic Immune ThrombocytoPenia + Case ReportDocument32 pagesChronic Immune ThrombocytoPenia + Case ReportSakada KokNo ratings yet
- Acute Appendicitis in Children - Diagnostic Imaging - UpToDateDocument28 pagesAcute Appendicitis in Children - Diagnostic Imaging - UpToDateHafiz Hari NugrahaNo ratings yet
- The Last SupperDocument27 pagesThe Last Supper2022: Valeria LievanoNo ratings yet
- Acute Pulmonary EmbolismDocument82 pagesAcute Pulmonary Embolismincredible Prages100% (1)
- ARDS Management Protocol: February 2018Document6 pagesARDS Management Protocol: February 2018soulstakers100% (1)
- Incarcerated Strangulated HerniaDocument12 pagesIncarcerated Strangulated HerniaamexatoNo ratings yet
- Glascow Coma ScaleDocument15 pagesGlascow Coma ScalePaul Henry RoxasNo ratings yet
- Case Presentation-1Document22 pagesCase Presentation-1srija vijjapuNo ratings yet
- Motion in 1 Dimension TestDocument11 pagesMotion in 1 Dimension TestKRISHNA KUTADINo ratings yet
- Telemedicine For Trauma, Emergencies and Disaster ManagementDocument58 pagesTelemedicine For Trauma, Emergencies and Disaster ManagementTransform Healthcare IT100% (1)
- Medicine I: 1.01 Patient Multipurpose Safety CurriculumDocument4 pagesMedicine I: 1.01 Patient Multipurpose Safety CurriculumDaniel EstradaNo ratings yet
- IM-Module B Summarized Notes (IBD)Document69 pagesIM-Module B Summarized Notes (IBD)DeepbluexNo ratings yet
- Sample Research ProposalDocument43 pagesSample Research ProposalLuis LazaroNo ratings yet
- Medical Doctor in Faculty of Medicine, University of Udayana, - Pulmonologist in Faculty of Medicine, University of Indonesia, JakartaDocument24 pagesMedical Doctor in Faculty of Medicine, University of Udayana, - Pulmonologist in Faculty of Medicine, University of Indonesia, Jakartazulfantri1983No ratings yet
- MechanicsDocument2 pagesMechanicsJonn Miguel GaabucayanNo ratings yet
- Nivetha Final Project 2Document81 pagesNivetha Final Project 2veena555No ratings yet
- Innovations in Cardiovascular Disease ManagementDocument183 pagesInnovations in Cardiovascular Disease ManagementGopal Kumar DasNo ratings yet
- Standard Surgical Attire Surgical ScrubDocument20 pagesStandard Surgical Attire Surgical ScrubzekkipianoNo ratings yet
- Easy Way To Interpret ABG ValuesDocument7 pagesEasy Way To Interpret ABG ValuesDoyTanNo ratings yet
- Revised Atlanta Classifi Cation ForDocument23 pagesRevised Atlanta Classifi Cation Forthalia reginoNo ratings yet
- Omphalocele and GastroschisisDocument12 pagesOmphalocele and Gastroschisisluisisea100% (1)
- Ventilator Graphics.Document69 pagesVentilator Graphics.LauraAlvarezMulett100% (2)
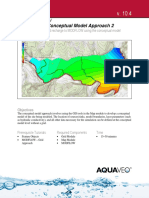
- Modflow - Conceptual Model Approach 2: GMS 10.4 TutorialDocument13 pagesModflow - Conceptual Model Approach 2: GMS 10.4 TutorialYetzabel FloresNo ratings yet
- Anatomy Important Images: AriseDocument14 pagesAnatomy Important Images: AriseadiNo ratings yet
- AlbuminDocument14 pagesAlbuminMaria Chona Penillos HularNo ratings yet
- Revised PCCP Spiro Consensus PDFDocument93 pagesRevised PCCP Spiro Consensus PDFJC ValenciaNo ratings yet
- ACLS Study Guide: New Updated 2015 AHA GuidelinesDocument33 pagesACLS Study Guide: New Updated 2015 AHA GuidelinesAdamRabbetNo ratings yet
- Chest PT in Icu 1996@609.full PDFDocument17 pagesChest PT in Icu 1996@609.full PDFDyah SafitriNo ratings yet
- Kuliayada CaafimaadkaDocument50 pagesKuliayada CaafimaadkaKhalid Abdiaziz AbdulleNo ratings yet
- modMODULE II-E DRUGS ACTING On NMJDocument6 pagesmodMODULE II-E DRUGS ACTING On NMJKenneth NuñezNo ratings yet
- DR Sandeep - EISENMENGER SYNDROMEDocument81 pagesDR Sandeep - EISENMENGER SYNDROMEAlexandrescuNo ratings yet
- Internal Medicine ACGME Program Requirements 2017-07-01Document43 pagesInternal Medicine ACGME Program Requirements 2017-07-01Amany SalamaNo ratings yet
- Chronic Venous InsufficiencyDocument4 pagesChronic Venous Insufficiencyfandi_cah_ganteng3367100% (1)
- Epi Confounding AssignmentDocument4 pagesEpi Confounding Assignmentcharles100% (2)
- LIGHT Pneumonia Dr. ConstantinoDocument6 pagesLIGHT Pneumonia Dr. ConstantinoMiguel Cuevas DolotNo ratings yet
- Nursing in EmergenciesDocument5 pagesNursing in EmergenciesAvisheel KalsiNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Building Utilities 06: Hope You Enjoyed The Quiz! Your Score Report Is Presented BelowDocument31 pagesBuilding Utilities 06: Hope You Enjoyed The Quiz! Your Score Report Is Presented BelowtriciasevenNo ratings yet
- PHILSCA Tops Aeronautical Board Exams Anew: Campus BeatDocument1 pagePHILSCA Tops Aeronautical Board Exams Anew: Campus BeatjiokoijikoNo ratings yet
- Capstone Project GuidelinesDocument23 pagesCapstone Project GuidelinesAdoree RamosNo ratings yet
- Advances in Emergent Airway Management in PediatricsDocument19 pagesAdvances in Emergent Airway Management in PediatricsLuis Miguel VillanuevaNo ratings yet
- Automatic Prediction of Diabetic Retinopathy and Glaucoma Through Retinal Image Analysis and Data Mining Techniques PDFDocument4 pagesAutomatic Prediction of Diabetic Retinopathy and Glaucoma Through Retinal Image Analysis and Data Mining Techniques PDFMohammad RofiiNo ratings yet
- Final Thesis 2018 08 23 18 13 33 319 PDFDocument69 pagesFinal Thesis 2018 08 23 18 13 33 319 PDFPriyanka KanodiaNo ratings yet
- 322 Copd Writing AssignmentDocument5 pages322 Copd Writing Assignmentapi-353335798No ratings yet
- CXR Interpretation: by Dr. Iqbal TariqDocument19 pagesCXR Interpretation: by Dr. Iqbal TariqSalman Khan100% (1)
- Asthma Phenotypes PDFDocument10 pagesAsthma Phenotypes PDFPhuong HuynhNo ratings yet
- AR 3 Airway Drug Assisted Intubation Protocol Final 2017 EditableDocument2 pagesAR 3 Airway Drug Assisted Intubation Protocol Final 2017 EditableAlejandroCabreraBustillo100% (1)
- An Updated Review of Hypertensive Emergencies and Urgencies: Katalin Makó, Corina Ureche, Zsuzsanna JeremiásDocument11 pagesAn Updated Review of Hypertensive Emergencies and Urgencies: Katalin Makó, Corina Ureche, Zsuzsanna JeremiásiganuryantiNo ratings yet
- PREM AlgorithmsDocument20 pagesPREM AlgorithmsalexNo ratings yet
- National TB ProgramDocument34 pagesNational TB ProgramASTR4 BABY100% (1)
- Template Trauma Long Case PresentationDocument1 pageTemplate Trauma Long Case PresentationAnonymous 4txA8N8etNo ratings yet
- Research Proposal Atrial Septal DefectDocument28 pagesResearch Proposal Atrial Septal DefectIzharIsmailNo ratings yet
- Soal-Soal Latihan: The Text Is For Question Number 1-6 The Princess and The PeaDocument3 pagesSoal-Soal Latihan: The Text Is For Question Number 1-6 The Princess and The PeaFilologus SiwabessyNo ratings yet
- Laryngomalacia PDFDocument6 pagesLaryngomalacia PDFFilologus SiwabessyNo ratings yet
- Status Pinguecula CHRDocument6 pagesStatus Pinguecula CHRFilologus SiwabessyNo ratings yet
- SasdaasdasdafasdfweDocument1 pageSasdaasdasdafasdfweFilologus SiwabessyNo ratings yet
- III. The Thousandfold ThoughtDocument251 pagesIII. The Thousandfold Thoughttareg4No ratings yet
- Viladimir PrinceDocument4 pagesViladimir PrinceSamNo ratings yet
- Locals 2012: HeritageDocument10 pagesLocals 2012: HeritageVCNews-BulletinNo ratings yet
- Guide To Reyes' Book (RPC II) Elements Et Al.Document13 pagesGuide To Reyes' Book (RPC II) Elements Et Al.Mariel Paulo LakayNo ratings yet
- The Easement Act, 1882Document2 pagesThe Easement Act, 1882MonzurNo ratings yet
- Ladonga VS., PeopleDocument3 pagesLadonga VS., PeopleAldrinmarkquintanaNo ratings yet
- Gebirgsjager FinalDocument72 pagesGebirgsjager FinalHetzer KrumNo ratings yet
- ZXXXXDocument2 pagesZXXXXwickedbootlegNo ratings yet
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-340713528No ratings yet
- Tutorial 3 (AIS)Document6 pagesTutorial 3 (AIS)Alan TingNo ratings yet
- Carlos Eenesto Valle Iglesias, A043 995 062 (BIA Sept. 18, 2013)Document3 pagesCarlos Eenesto Valle Iglesias, A043 995 062 (BIA Sept. 18, 2013)Immigrant & Refugee Appellate Center, LLCNo ratings yet
- 1 TimothyDocument14 pages1 TimothyThomas Nelson Bibles100% (3)
- (NEW DJ) Hill, Et Al. v. Bakersfield Police Department - Document No. 4Document1 page(NEW DJ) Hill, Et Al. v. Bakersfield Police Department - Document No. 4Justia.comNo ratings yet
- Catholic Social Teaching Power Point Chapter 1Document23 pagesCatholic Social Teaching Power Point Chapter 1Jimmy Yau0% (1)
- Bar Council of Indias Rules For Registration and Regulation of Foreign Lawyers and Foreign Law Firms in India 2023Document7 pagesBar Council of Indias Rules For Registration and Regulation of Foreign Lawyers and Foreign Law Firms in India 2023bhavsar20190401066No ratings yet
- LEGAL IMPEDIMENTS ON THE PRACTICAL IMPLEMENTATION OF THE CHILD RIGHT ACT 2003 by Akin Olawale OgundayisiDocument16 pagesLEGAL IMPEDIMENTS ON THE PRACTICAL IMPLEMENTATION OF THE CHILD RIGHT ACT 2003 by Akin Olawale OgundayisiAkin Olawale Oluwadayisi100% (1)
- Summary of The Second CrusadeDocument2 pagesSummary of The Second CrusadeMeweranNo ratings yet
- Students Speech TopicsDocument5 pagesStudents Speech TopicsManar AdelNo ratings yet
- Edit Item DataDocument4 pagesEdit Item Datachaosraven42099No ratings yet
- Torts Digests San Beda Alabang 2011Document171 pagesTorts Digests San Beda Alabang 2011Angela Marie Alfaro Pascual100% (3)
- 110-Balgos Vs SandiganbayanDocument2 pages110-Balgos Vs SandiganbayanAlexis Ailex Villamor Jr.No ratings yet
- Americas 200 Year Old War With IslamDocument31 pagesAmericas 200 Year Old War With IslamGary Bautista PeredoNo ratings yet
- 250 VerbsDocument24 pages250 VerbsKonul AllahverdiyevaNo ratings yet
- Ship OrganizationDocument3 pagesShip OrganizationJj GonzalesNo ratings yet
- External Review Into Sexual Misconduct and Sexual Harassment in The Canadian Armed ForcesDocument107 pagesExternal Review Into Sexual Misconduct and Sexual Harassment in The Canadian Armed Forcesapi-261753894No ratings yet
- Summary Judgment (Order 14) & Its Preliminary Requirement: HJH Zalwatul Sakinah HJ Ibrahim 13B0204Document11 pagesSummary Judgment (Order 14) & Its Preliminary Requirement: HJH Zalwatul Sakinah HJ Ibrahim 13B0204Zall IbrahimNo ratings yet
- Child LabourDocument3 pagesChild LabourHimani ShahNo ratings yet