You might also like
- Blueprints of Cosmic Consciousness Book 1Document129 pagesBlueprints of Cosmic Consciousness Book 1Donald William50% (2)
- Handbook of Biblical Criticism by Richard N Soulen 4th Edition PDFDocument268 pagesHandbook of Biblical Criticism by Richard N Soulen 4th Edition PDFHezekiah Walker83% (6)
- Algorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFDocument6 pagesAlgorithms For IV Fluid Therapy in Children and Young People in Hospital Set of 6 PDF 2190274957 PDFFurqon AfandriNo ratings yet
- Jurnal PEIDocument4 pagesJurnal PEIMadonna Frozen100% (1)
- Pile Design Report by RANR RanasingheDocument45 pagesPile Design Report by RANR Ranasinghelvsw1100% (1)
- Induction of Labor With Oxytocin - UpToDateDocument54 pagesInduction of Labor With Oxytocin - UpToDateJhoseline CamposNo ratings yet
- Draft Share Purchase AgreementDocument30 pagesDraft Share Purchase AgreementAkshayaAgarwal100% (1)
- Teacher Guide: No Bill of Rights, No DealDocument16 pagesTeacher Guide: No Bill of Rights, No DealEmily100% (1)
- eEMCASE - MAR Letak Rendah Tanpa FistelDocument22 pageseEMCASE - MAR Letak Rendah Tanpa FistelashyNo ratings yet
- Kardiotokografi Ppds (DR - JKS)Document68 pagesKardiotokografi Ppds (DR - JKS)Aditya PrabawaNo ratings yet
- Adrianes Bachnas - Preeclampsia Screening Algorythm 2Document23 pagesAdrianes Bachnas - Preeclampsia Screening Algorythm 2Wienda GeraldineNo ratings yet
- Chapter 14Document26 pagesChapter 14Sharonz MuthuveeranNo ratings yet
- Physiology of Micturition ReflexDocument37 pagesPhysiology of Micturition ReflexPhysiology by Dr Raghuveer100% (13)
- Vitamin DDocument2 pagesVitamin DAdrianne BazoNo ratings yet
- Terapi Lesi Pra-Kanker Leher Rahim (Krioterapi)Document31 pagesTerapi Lesi Pra-Kanker Leher Rahim (Krioterapi)yulia gustiNo ratings yet
- DR Rosi - Nec Free NicuDocument51 pagesDR Rosi - Nec Free NicukemalahmadNo ratings yet
- Embriologi GinjalDocument39 pagesEmbriologi GinjalUttari DalemNo ratings yet
- (PPT) Superimposed Hypertension in PregnancyDocument37 pages(PPT) Superimposed Hypertension in PregnancyTimotius Wira YudhaNo ratings yet
- PEOPLE v. OLIVAREZDocument1 pagePEOPLE v. OLIVAREZBaphomet Junior100% (1)
- Lapkas Hymen ImperforataDocument27 pagesLapkas Hymen ImperforataKhairida Hafni LbsNo ratings yet
- Austin Journal of Anesthesia and AnalgesiaDocument3 pagesAustin Journal of Anesthesia and AnalgesiaAustin Publishing GroupNo ratings yet
- Ats Menjawab Soal Gin Nov21 Final 50Document14 pagesAts Menjawab Soal Gin Nov21 Final 50anton suponoNo ratings yet
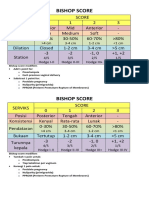
- Bishop ScoreDocument2 pagesBishop ScoreRskia Sadewwa Yogyakarta100% (1)
- Sarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalDocument2 pagesSarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalTan Chin AunNo ratings yet
- Akreditasi Trisakti PDFDocument1 pageAkreditasi Trisakti PDFMargaret SimmonsNo ratings yet
- Disproporsi Kepala PanggulDocument14 pagesDisproporsi Kepala PanggulIntan PermataNo ratings yet
- Skor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermDocument9 pagesSkor Bishop, Profil Biofisik Janin, Dan Tanda Kehamilan Post-TermMuhammad KhoiruddinNo ratings yet
- Janica E. Walden, MD Neuroradiology University of North CarolinaDocument21 pagesJanica E. Walden, MD Neuroradiology University of North CarolinaBilly ChietraNo ratings yet
- GestosisDocument12 pagesGestosisravannofanizzaNo ratings yet
- Gannguan PubertasDocument56 pagesGannguan PubertasAde Yosdi PutraNo ratings yet
- Ogilvie SyndromeDocument8 pagesOgilvie SyndromeMuhammad FaisalNo ratings yet
- Jadwal Acara PIT POGI 25 Padang Update 3 Sept 2021Document8 pagesJadwal Acara PIT POGI 25 Padang Update 3 Sept 2021daniel_alexander_susenoNo ratings yet
- Tugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiDocument3 pagesTugas SC Vs Histerotomi Vs Laparotomi Ambil Anak Aji PatriajatiAji PatriajatiNo ratings yet
- Babygram PDFDocument22 pagesBabygram PDFArtikelWanitaDanKehamilanNo ratings yet
- Telaah Kritis JurnalDocument13 pagesTelaah Kritis JurnalfebrinaNo ratings yet
- Tatalaksana Terkini Cedera Ginjal AkutDocument25 pagesTatalaksana Terkini Cedera Ginjal AkutSulistyawati WrimunNo ratings yet
- Abdominal Pain in Children - Dr. Hermanto SP - BaDocument41 pagesAbdominal Pain in Children - Dr. Hermanto SP - Bajimmy_junNo ratings yet
- Morning Report ObsgynDocument30 pagesMorning Report ObsgynGema Akbar WakhidanaNo ratings yet
- Anemia Prenatal Care - DR - Rima IrwindaDocument43 pagesAnemia Prenatal Care - DR - Rima IrwindaHari SandiNo ratings yet
- The Occiput Posterior Fetus: Oleh: Wiliyanto. Wijaya Pembimbing: Dr. Ims Murah Manoe, Spog (K)Document24 pagesThe Occiput Posterior Fetus: Oleh: Wiliyanto. Wijaya Pembimbing: Dr. Ims Murah Manoe, Spog (K)Eka KurniatiNo ratings yet
- Materi EbookDocument11 pagesMateri EbookRisky UntariNo ratings yet
- Z Scores GirlsDocument7 pagesZ Scores GirlsJames Karl HugoNo ratings yet
- Ekstraksi Forceps Vacuum Mahasiswa Fkui TK ViDocument19 pagesEkstraksi Forceps Vacuum Mahasiswa Fkui TK ViCiiezz BunciiezzNo ratings yet
- Mnemonic Vacum Dan Forcep NewDocument2 pagesMnemonic Vacum Dan Forcep NewsinggehNo ratings yet
- Placental PathologyDocument465 pagesPlacental PathologyOana Roxana PuscasNo ratings yet
- Jurnal Plasenta Akreta PDFDocument5 pagesJurnal Plasenta Akreta PDFfatqur28No ratings yet
- Retractile TestisDocument7 pagesRetractile TestisAhmad Rahmat Ramadhan TantuNo ratings yet
- Implantation and Development Placenta Part 2Document36 pagesImplantation and Development Placenta Part 2Tengku Chairannisa PutriNo ratings yet
- 1157 - Basic Ecg Dr. Ragil Nur Rosyadi, SPJP, FihaDocument74 pages1157 - Basic Ecg Dr. Ragil Nur Rosyadi, SPJP, FihaSibro Malisi100% (1)
- BB Increment GIRLS PDFDocument1 pageBB Increment GIRLS PDFrendyNo ratings yet
- Tanner StageDocument6 pagesTanner StageSitaNo ratings yet
- Rectovagina FistulaDocument13 pagesRectovagina FistulaNurul HikmahNo ratings yet
- Fetal Neural Tube 2021 12 LMBR PDFDocument24 pagesFetal Neural Tube 2021 12 LMBR PDFwayansiagaNo ratings yet
- Case Distosia Bahu Fix (Repaired)Document18 pagesCase Distosia Bahu Fix (Repaired)Vhandy RamadhanNo ratings yet
- Corpus Alienum EsophagusDocument3 pagesCorpus Alienum EsophagusTrhey Ahmilza DamaitaNo ratings yet
- HipospadiaDocument66 pagesHipospadiaDichaNo ratings yet
- Fisiologi DefekasiDocument9 pagesFisiologi DefekasiAmirullah AbdiNo ratings yet
- Pemeriksaan Foto Thorax Pada Anak-AnakDocument29 pagesPemeriksaan Foto Thorax Pada Anak-AnakRenaldy PamungkasNo ratings yet
- AUB Current Update (Malam Keakraban PAOGI)Document36 pagesAUB Current Update (Malam Keakraban PAOGI)armillaraissyaNo ratings yet
- Proses Persalinan Dan Konsep DasarDocument31 pagesProses Persalinan Dan Konsep DasarShella Ramashanti100% (1)
- Anatomi Panggul, Sistem Hormonal Dan Konsepsi: Ns. Dina Mariyana.,S.KepDocument56 pagesAnatomi Panggul, Sistem Hormonal Dan Konsepsi: Ns. Dina Mariyana.,S.KepAna KareniaNo ratings yet
- What Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)Document39 pagesWhat Do We Know About Patent Dustus Arteriosus - Dr. Adhi Teguh, Sp.a (K)laurentiaNo ratings yet
- Mola Hidantidosa & Gestational Trophoblastic NeoplasmaDocument23 pagesMola Hidantidosa & Gestational Trophoblastic NeoplasmanurkamilawatiNo ratings yet
- tuGAS KILOTHORAXDocument25 pagestuGAS KILOTHORAXAlma WijayaNo ratings yet
- Anatomi PanggulDocument34 pagesAnatomi PanggulKhodijahNo ratings yet
- Klasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015Document3 pagesKlasifikasi Tumor Paru Secara Histologis Menurut WHO Tahun 2015lindaNo ratings yet
- Gastroschizis Vs OmfalocelDocument35 pagesGastroschizis Vs OmfalocelElena LicsandruNo ratings yet
- Urinary Incontinence: Genet Gebremedhin (MD) April 4 2017Document34 pagesUrinary Incontinence: Genet Gebremedhin (MD) April 4 2017bemnetNo ratings yet
- Chapter 1 Lecture NotesDocument12 pagesChapter 1 Lecture NotesRachel FreemanNo ratings yet
- 201 359 1 SMDocument18 pages201 359 1 SMAli SodikinNo ratings yet
- English For Specific Purposes SyllabusDocument12 pagesEnglish For Specific Purposes Syllabus다옌No ratings yet
- Senior High School The Problem and Review of Related LiteratureDocument13 pagesSenior High School The Problem and Review of Related LiteratureJayveelyn Clamonte100% (1)
- Lads Jacking MethodDocument2 pagesLads Jacking MethodDarren I'am TroginsNo ratings yet
- Word-Formation-30t4-2017 L P 10Document4 pagesWord-Formation-30t4-2017 L P 10Yen LamNo ratings yet
- In The West, The Shadow of The Gnomon Points East (As Shown in The Pictures Below)Document7 pagesIn The West, The Shadow of The Gnomon Points East (As Shown in The Pictures Below)ShanmugasundaramNo ratings yet
- Understanding Educational Technology: Its Nature and CharacteristicsDocument3 pagesUnderstanding Educational Technology: Its Nature and CharacteristicsKim NoblezaNo ratings yet
- Cara Penulisan Nota Kaki (Footnote) Dan BibliografiDocument3 pagesCara Penulisan Nota Kaki (Footnote) Dan BibliografiChloeLeeNo ratings yet
- Radius Manager GuideDocument73 pagesRadius Manager GuideAlex KobeissyNo ratings yet
- Conceptual FrameworkDocument1 pageConceptual FrameworkthestroNo ratings yet
- Metodos de Ensayo Ash ProbeDocument5 pagesMetodos de Ensayo Ash ProbediegoNo ratings yet
- NCERT Class 12 BiologyDocument311 pagesNCERT Class 12 BiologySincerely YoursNo ratings yet
- ATM For 3G - NSNDocument50 pagesATM For 3G - NSNEko MardiantoNo ratings yet
- Paleth ReportDocument51 pagesPaleth ReportMarlon Rey AnacletoNo ratings yet
- Reflective EssayDocument3 pagesReflective Essayapi-242212904100% (1)
- Manual Mikrotik Rb450gx4Document3 pagesManual Mikrotik Rb450gx4um4irNo ratings yet
- My Final Research PaperDocument23 pagesMy Final Research PaperyenpalerNo ratings yet
- Tauhid Islamic Monotheism.Document2 pagesTauhid Islamic Monotheism.Mikel AlonsoNo ratings yet
- Project Report Guidelines Canvas StudentDocument17 pagesProject Report Guidelines Canvas StudentMrunalini KhandareNo ratings yet
- Biodegradation of Metallic Surgical Implants Investigated Using Anultrasound-Assisted Process Combined With ICP-OES and XRDDocument5 pagesBiodegradation of Metallic Surgical Implants Investigated Using Anultrasound-Assisted Process Combined With ICP-OES and XRDmustafaNo ratings yet
- Prescription 1691038324139Document7 pagesPrescription 1691038324139abhishekt4xNo ratings yet