You might also like
- Kenya Immunization ScheduleDocument1 pageKenya Immunization ScheduleDani AnyikaNo ratings yet
- TularemiaDocument19 pagesTularemiaEmily EresumaNo ratings yet
- Hydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Document40 pagesHydrocephalus: I Dewa Ketut Gede Herry Oka Pembimbing: Dr. Dr. I Wayan Niryana, Sp. BS (K)Dewa Oka100% (1)
- Journal ReadingDocument19 pagesJournal ReadingSarah SiraitNo ratings yet
- Meningitis: Shafaat Ullah BSN. Gen Khyber Medical UniversityDocument18 pagesMeningitis: Shafaat Ullah BSN. Gen Khyber Medical UniversityAbdirahman Abdillahi Farah100% (1)
- 2018 - Dr. Mahatma - Syndrome MetabolikDocument79 pages2018 - Dr. Mahatma - Syndrome MetabolikDEWI MULYANINo ratings yet
- OSCE Checklist Newborn Baby Assessment NIPEDocument3 pagesOSCE Checklist Newborn Baby Assessment NIPETauqeer Ahmed0% (1)
- Neonatal SepsisDocument47 pagesNeonatal SepsisThea Dino100% (1)
- Case Study On LBWDocument43 pagesCase Study On LBWOmotosho Alex50% (2)
- Natures Hidden Health MiracleDocument38 pagesNatures Hidden Health MiracleGorneau100% (2)
- Aapc 2016Document92 pagesAapc 2016Ravi Pal75% (4)
- N.sepsis 2Document129 pagesN.sepsis 2cooldude_secbad1712100% (1)
- Necrotizing Enterocolotis (NEC)Document2 pagesNecrotizing Enterocolotis (NEC)JDRN14No ratings yet
- NBS Law FinalDocument33 pagesNBS Law Finalkissiah Cajetas100% (1)
- Preterm+Prelabour+Rupture+of+the+Membranes Sept2015Document12 pagesPreterm+Prelabour+Rupture+of+the+Membranes Sept2015molenNo ratings yet
- Respiratory Distress Syndrome: Islamic University Nursing CollegeDocument21 pagesRespiratory Distress Syndrome: Islamic University Nursing Collegeyaumil agisnaNo ratings yet
- Neonatal JaundiceDocument63 pagesNeonatal JaundiceMade Oka HeryanaNo ratings yet
- NN Jaundice - MoteeDocument70 pagesNN Jaundice - MoteeMhmNo ratings yet
- 2 NewbornDocument123 pages2 NewbornANNIE SHINE MAGSACAYNo ratings yet
- Necrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualDocument3 pagesNecrotizing Enterocolitis (NEC) : Intensive Care Nursery House Staff ManualJovvitaNo ratings yet
- Makalah Evidence Based MedicineDocument14 pagesMakalah Evidence Based MedicineanggidinataNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document24 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)hendra2darmawanNo ratings yet
- Genitourinary TuberculosisDocument24 pagesGenitourinary TuberculosisAndre F SusantioNo ratings yet
- E Posters PDFDocument349 pagesE Posters PDFpriyadikkalaNo ratings yet
- Neonatal JaundiceDocument23 pagesNeonatal JaundiceAsad M AminNo ratings yet
- Clinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineDocument10 pagesClinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineUtomo BudidarmoNo ratings yet
- VAP SlidesDocument25 pagesVAP SlidesGladys OliviaNo ratings yet
- HepatosplenomegalyDocument49 pagesHepatosplenomegalyTarun SinghNo ratings yet
- Botulism 08.16.2013Document12 pagesBotulism 08.16.2013Emily EresumaNo ratings yet
- Ptl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureDocument38 pagesPtl/Pprom and Multifetal Gestation: Anna Buabbud MD Ms3 LectureNik C0% (1)
- TORCH InfectionsDocument37 pagesTORCH InfectionsEylin Halim Rahardjo100% (1)
- Celiac DiseaseDocument33 pagesCeliac Diseasevalika_c100% (1)
- Pa Tho PhysiologyDocument4 pagesPa Tho Physiologyimagine28No ratings yet
- Hisprung DiseaseDocument12 pagesHisprung DiseaseEky Madyaning NastitiNo ratings yet
- Tuberculosis: Muhammad IqbalDocument16 pagesTuberculosis: Muhammad Iqbalvictor dadaNo ratings yet
- Hydranencephaly ManagementDocument20 pagesHydranencephaly ManagementJohn Christopher LucesNo ratings yet
- Breast Cancer: Dr. Armando V. Tan AnatomyDocument9 pagesBreast Cancer: Dr. Armando V. Tan AnatomyJennifer Dumaluan AtaNo ratings yet
- Henoch Schonlein Purpura REVDocument42 pagesHenoch Schonlein Purpura REVBayu Kurniawan100% (1)
- IKD 2 - Imaging Renal InfectionDocument49 pagesIKD 2 - Imaging Renal InfectionRenal Association MauritiusNo ratings yet
- Perinatal InfectionsDocument24 pagesPerinatal InfectionsAlexandra OanaNo ratings yet
- Basic Physical Examination In: UrologyDocument55 pagesBasic Physical Examination In: Urologyradiaputri25No ratings yet
- Zebras of Neonatal Hypoglycemia 06.09.2014Document21 pagesZebras of Neonatal Hypoglycemia 06.09.2014Emily EresumaNo ratings yet
- Final Update On Antenatal Steroids - DR PadmeshDocument66 pagesFinal Update On Antenatal Steroids - DR PadmeshAhalia NicuNo ratings yet
- Maisel S 2012Document5 pagesMaisel S 2012marsyaNo ratings yet
- Acute Abdomen SummaryDocument3 pagesAcute Abdomen SummaryAbdul Ghaffar AbdullahNo ratings yet
- Preoperative Assessment Hairina MazlanDocument27 pagesPreoperative Assessment Hairina MazlanHairina MazlanNo ratings yet
- Clinical Cases in Microbiology and Infectious Disease - SAFMLS (PDFDrive)Document172 pagesClinical Cases in Microbiology and Infectious Disease - SAFMLS (PDFDrive)Dana MontenegroNo ratings yet
- Written2 ADocument5 pagesWritten2 Aivan_gunawan_9No ratings yet
- Neonatal ProceduresDocument74 pagesNeonatal ProceduresIbrahim Sabra100% (1)
- Newborn Screening: Alyssa Nicole B. ReyesDocument12 pagesNewborn Screening: Alyssa Nicole B. ReyesJohn Christian LasalitaNo ratings yet
- TLD Transition Slides - Oct 2018Document18 pagesTLD Transition Slides - Oct 2018SemeeeJuniorNo ratings yet
- H.influenzae Modified 2012Document12 pagesH.influenzae Modified 2012MoonAIRNo ratings yet
- S2HY SlideHandoutsDocument511 pagesS2HY SlideHandoutsDorin Cristian AntalNo ratings yet
- 2022 Ob2 s1t15 Preterm Labor and BirthDocument12 pages2022 Ob2 s1t15 Preterm Labor and BirthmedicoNo ratings yet
- Recent Update in The Management of Invasive Fungal InfectionDocument30 pagesRecent Update in The Management of Invasive Fungal Infectionanoop61100% (2)
- Host Microbe InteractionsDocument51 pagesHost Microbe InteractionsIsworo RukmiNo ratings yet
- Respiratory Distress in Newborn FinalDocument22 pagesRespiratory Distress in Newborn FinalajayganeshjNo ratings yet
- NEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaDocument18 pagesNEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaGaluh Martin MaytasariNo ratings yet
- Case Report "Febrile Seizures": Betsheba E. S. 123307018Document37 pagesCase Report "Febrile Seizures": Betsheba E. S. 123307018AmandaRizkaNo ratings yet
- OBG Revision 15 Year UPSC CMSDocument63 pagesOBG Revision 15 Year UPSC CMSbithika pathakNo ratings yet
- Constipation in ChildrenDocument34 pagesConstipation in Childrenabdisalaan hassanNo ratings yet
- MusQan National Quality Assurance Standards and Assessment Tools For DH and CHCDocument274 pagesMusQan National Quality Assurance Standards and Assessment Tools For DH and CHCRahul JalauniaNo ratings yet
- The Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesFrom EverandThe Ideal Neutropenic Diet Cookbook; The Super Diet Guide To Replenish Overall Health For A Vibrant Lifestyle With Nourishing RecipesNo ratings yet
- Investigatory Project On AnalgesicsDocument30 pagesInvestigatory Project On AnalgesicsAnurag Singh100% (1)
- Optic Atrophy :major Review March 2010, Kerala Journal of Ophthalmology, Devendra V. Venkatramani Et AlDocument6 pagesOptic Atrophy :major Review March 2010, Kerala Journal of Ophthalmology, Devendra V. Venkatramani Et AlNavojit ChowdhuryNo ratings yet
- Jurnal Kesehatan Dr. SoebandiDocument6 pagesJurnal Kesehatan Dr. SoebandiHary BudiartoNo ratings yet
- Jurnal PterigiumDocument6 pagesJurnal PterigiumMonica Lauretta Sembiring IINo ratings yet
- Optic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsDocument5 pagesOptic Nerve Glioma: Case Series With Review of Clinical, Radiologic, Molecular, and Histopathologic CharacteristicsUtama Hadiputra SurbaktiNo ratings yet
- 5 - Formal ReportDocument16 pages5 - Formal ReportJacob MarczakNo ratings yet
- Astrazenica 2nd Dose 8-13-21 AlkieDocument109 pagesAstrazenica 2nd Dose 8-13-21 AlkieGanie Mar BiasonNo ratings yet
- Prosthetic Case PresentationsDocument19 pagesProsthetic Case PresentationsptannenbaumNo ratings yet
- FHSISDocument15 pagesFHSISThon Lopez MagpantayNo ratings yet
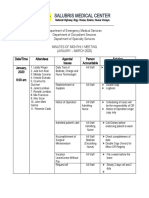
- Salubris Medical Center: National Highway, Brgy. Roxas, Solano, Nueva VizcayaDocument10 pagesSalubris Medical Center: National Highway, Brgy. Roxas, Solano, Nueva Vizcayajulie ann afanNo ratings yet
- Paper 1Document11 pagesPaper 1api-499574410No ratings yet
- New Techniques in Chelonian Shell RepairDocument8 pagesNew Techniques in Chelonian Shell RepairChecko LatteNo ratings yet
- Aga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsDocument15 pagesAga Khan University Postgraduate Medical Education (Pgme) Induction Frequently Asked QuestionsRamzan BibiNo ratings yet
- PhotodermatosesDocument8 pagesPhotodermatosesIvan KurniadiNo ratings yet
- Refractive Surgery Standards Dec 2004Document7 pagesRefractive Surgery Standards Dec 2004dr_jrcNo ratings yet
- Notes On MRI - FinalDocument16 pagesNotes On MRI - FinalAnju GuptaNo ratings yet
- How Do I Know If My Activities Are of Moderate To Vigorous Intensity?Document2 pagesHow Do I Know If My Activities Are of Moderate To Vigorous Intensity?Balsc Bals BalscNo ratings yet
- Cps-Pg-Admission-2019 First Selection Round of Neet Eligible Candidates For The State of MaharashtraDocument93 pagesCps-Pg-Admission-2019 First Selection Round of Neet Eligible Candidates For The State of MaharashtrarohankananiNo ratings yet
- The Effects of Exercise On The Nervous SystemDocument2 pagesThe Effects of Exercise On The Nervous SystemramadanNo ratings yet
- Essentials of Diagnosis, Treatment, and Application of Cardiac and Peripheral Vascular DiseasesDocument295 pagesEssentials of Diagnosis, Treatment, and Application of Cardiac and Peripheral Vascular DiseasesMichael BrunetNo ratings yet
- DEPRESSANTSDocument18 pagesDEPRESSANTSElisha Arwynne Postrero RomaNo ratings yet
- Dr. Otman Siregar, Spot, (K) Spine Ilmu Bedah Orthopaedi Fk-Usu/Rsup Ham 2010Document53 pagesDr. Otman Siregar, Spot, (K) Spine Ilmu Bedah Orthopaedi Fk-Usu/Rsup Ham 2010yuliaoksiyulanda ingeniopadangNo ratings yet
- Mechanisms of Dry Needling and Diff BW AccDocument4 pagesMechanisms of Dry Needling and Diff BW AccVardhman Jain100% (1)
- JednjakDocument15 pagesJednjakbojana1994No ratings yet
- Blaylock Forced0415 130Document13 pagesBlaylock Forced0415 130RAMO STEF SZEKERESNo ratings yet
- Powerpoint TaeniasisDocument23 pagesPowerpoint TaeniasisAyshaShariff0% (1)
- Head Nurse Experience (Staffing)Document3 pagesHead Nurse Experience (Staffing)Abigail BrillantesNo ratings yet