You might also like
- Complete Denture EstheticsDocument14 pagesComplete Denture Estheticsdrreba100% (5)
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Patients Complaints Following Partial Denture InsertionDocument50 pagesPatients Complaints Following Partial Denture InsertionHector Sa50% (2)
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- The Importance of the Posterior Palatal Seal in Complete DenturesDocument48 pagesThe Importance of the Posterior Palatal Seal in Complete Denturesneeha_mds100% (2)
- Immediate DenturesDocument35 pagesImmediate DenturesSimran SahniNo ratings yet
- Fixed Prosthodontics in Dental PracticeFrom EverandFixed Prosthodontics in Dental PracticeRating: 4 out of 5 stars4/5 (1)
- Complete Denture Case History ProformaDocument8 pagesComplete Denture Case History ProformaMrunal Doiphode100% (2)
- Partial Coverage PPT FinalDocument83 pagesPartial Coverage PPT FinalTotta Ayman50% (2)
- Adhesive Restoration of Endodontically Treated TeethFrom EverandAdhesive Restoration of Endodontically Treated TeethRating: 3 out of 5 stars3/5 (2)
- Overdenture Presentation PDFDocument19 pagesOverdenture Presentation PDFAjay Mehta100% (1)
- The Complete Guide to Dental Implants: All About DentistryFrom EverandThe Complete Guide to Dental Implants: All About DentistryNo ratings yet
- ObturatorDocument15 pagesObturatorFarhan Kabeer100% (1)
- OVERDENTURESDocument15 pagesOVERDENTURESAditya SavirmathNo ratings yet
- Operative Dentistry in the Phantom LabFrom EverandOperative Dentistry in the Phantom LabRating: 5 out of 5 stars5/5 (1)
- Esthetics in FPD Seminaar 7Document71 pagesEsthetics in FPD Seminaar 7DrFarha Naz100% (1)
- Swing Lock Partial DentureDocument22 pagesSwing Lock Partial DentureSanNo ratings yet
- OBTURATORSDocument69 pagesOBTURATORSSecret OriginsNo ratings yet
- RPD Manual 2013-2014 FinalDocument76 pagesRPD Manual 2013-2014 Finalpriyamjani100% (4)
- Maxillofacial ProstheticsDocument7 pagesMaxillofacial ProstheticsAmar Bhochhibhoya100% (1)
- Radiographs in Prosthodontics / Orthodontic Courses by Indian Dental AcademyDocument38 pagesRadiographs in Prosthodontics / Orthodontic Courses by Indian Dental Academyindian dental academy100% (4)
- Prostho Rehabilitation - HypodontiaDocument24 pagesProstho Rehabilitation - HypodontiaAmniAzmiNo ratings yet
- Materials Used in Maxillofacial ProsthesisDocument88 pagesMaterials Used in Maxillofacial ProsthesisAkanksha MahajanNo ratings yet
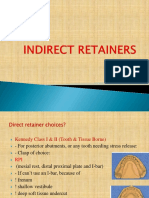
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Occlusal Relationship in RPD ProsthoDocument23 pagesOcclusal Relationship in RPD ProsthoFourthMolar.com100% (3)
- Failures in Removable Partial DentureDocument78 pagesFailures in Removable Partial DenturePrabhu Raj Singh100% (3)
- Abutment Selection in Fixed Partial Denture PDFDocument6 pagesAbutment Selection in Fixed Partial Denture PDFheycoolalexNo ratings yet
- Finish Line of The Preparation Is The End of Tooth PreparationDocument36 pagesFinish Line of The Preparation Is The End of Tooth PreparationAnureet MehrokNo ratings yet
- SplintsDocument3 pagesSplintsmuhammad naeem50% (2)
- Guide to Managing Flabby Ridges and Hypertrophic TissuesDocument145 pagesGuide to Managing Flabby Ridges and Hypertrophic TissuesJudy Abbott100% (1)
- Working Cast and DieDocument47 pagesWorking Cast and DieFira Maminya Maurah0% (1)
- Diagnostic Aids in ProsthodonticsDocument60 pagesDiagnostic Aids in ProsthodonticsAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Steps to Fabricating a Removable Partial DentureDocument27 pagesSteps to Fabricating a Removable Partial DentureAmita100% (2)
- OverdentureDocument227 pagesOverdentureEazhil RajNo ratings yet
- Harry Diagnostic Wax-UpDocument41 pagesHarry Diagnostic Wax-Uprema100% (4)
- Immediate Dentures - S2Document41 pagesImmediate Dentures - S2Nikita AggarwalNo ratings yet
- Preventive ProsthodonticsDocument13 pagesPreventive Prosthodonticsbhuvanesh4668100% (1)
- Jaw RelationsDocument12 pagesJaw RelationsZhuoYuan HowNo ratings yet
- Relining & RebasingDocument86 pagesRelining & RebasingJASPREETKAUR0410100% (1)
- Retainers in FPDDocument153 pagesRetainers in FPDAmit Bhargav88% (8)
- RPD Wax-Up TechniquesDocument4 pagesRPD Wax-Up Techniqueshan1491100% (1)
- Principles of Tooth PreparationDocument43 pagesPrinciples of Tooth PreparationJyoti Raheja100% (3)
- CD Bernard LevinDocument172 pagesCD Bernard LevinIndrani Das50% (2)
- Complete Denture Occlusion PDFDocument25 pagesComplete Denture Occlusion PDFÄpriolia SuNo ratings yet
- Classification of Failure of FPDDocument4 pagesClassification of Failure of FPDrayavarapu sunilNo ratings yet
- Balancing Ramps in Nonanatomic Complete DentureDocument3 pagesBalancing Ramps in Nonanatomic Complete DentureDron Lakhani100% (4)
- 1 Laboratory Procedures RPDDocument30 pages1 Laboratory Procedures RPDJASPREETKAUR0410100% (4)
- CD Qa1Document5 pagesCD Qa1DontoNo ratings yet
- Impression in FPDDocument9 pagesImpression in FPDAmar Bhochhibhoya100% (1)
- Retainers in FPDDocument32 pagesRetainers in FPDPriyanthi A50% (2)
- Provisionals in Dentistry - From Past To Recent Advances: Rohitraghavan, Shajahan P A, NeenakunjumonDocument6 pagesProvisionals in Dentistry - From Past To Recent Advances: Rohitraghavan, Shajahan P A, Neenakunjumonnavdeep100% (1)
- Concepts of Complete Denture OcclusionDocument39 pagesConcepts of Complete Denture Occlusionaziz2007100% (1)
- Stress Breakers: DR Mayur HegdeDocument35 pagesStress Breakers: DR Mayur HegdeSan0% (1)
- ObturatorsDocument79 pagesObturatorsPremshith CpNo ratings yet
- Esthetic in Complete DentureDocument14 pagesEsthetic in Complete DentureNidhi KatochNo ratings yet
- Casted Post CoreDocument8 pagesCasted Post CoreMadSadNo ratings yet
- Textbook of Orthodontics Samir Bishara 599 52MB 401 407Document7 pagesTextbook of Orthodontics Samir Bishara 599 52MB 401 407Ortodoncia UNAL 2020No ratings yet
- Diagnostic Elements For Tooth Extraction in OrthodonticsDocument24 pagesDiagnostic Elements For Tooth Extraction in OrthodonticsLanaNo ratings yet
- Retention and Stability: A Review of The LiteratureDocument8 pagesRetention and Stability: A Review of The LiteratureLanaNo ratings yet
- Orthognathic SurgeryDocument26 pagesOrthognathic Surgerym.n.n .q.c.fNo ratings yet
- Twin Blocks Combined with Orthopedic Traction Effectively Treat Class II MalocclusionsDocument8 pagesTwin Blocks Combined with Orthopedic Traction Effectively Treat Class II MalocclusionsAnupamaNo ratings yet
- Understanding Anchorage in Orthodontics-Review ArticlesDocument5 pagesUnderstanding Anchorage in Orthodontics-Review ArticlesSoe San KyawNo ratings yet
- Clear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewDocument4 pagesClear Aligners, A Milestone in Invisible Orthodontics - A Literature ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Eastman PDFDocument7 pagesEastman PDFMonojit DuttaNo ratings yet
- Laura Mitchell - An Introduction To Orthodontics-Oxford University Press (2013) PDFDocument326 pagesLaura Mitchell - An Introduction To Orthodontics-Oxford University Press (2013) PDFGavrilescu Mihai84% (25)
- Finishing Stage Maxillary Cant CorrectionDocument132 pagesFinishing Stage Maxillary Cant Correctionsahar emadNo ratings yet
- Exposé 2Document16 pagesExposé 2PoNo ratings yet
- Early Orthodontic Treatment: What Are The Imperatives?: Journal of The American Dental Association (1939) June 2000Document10 pagesEarly Orthodontic Treatment: What Are The Imperatives?: Journal of The American Dental Association (1939) June 2000Javier Farias VeraNo ratings yet
- Fixed Functional ApplianceDocument71 pagesFixed Functional AppliancekpNo ratings yet
- 18.a Cephalometric Evaluation of Tongue From The Rest Position To Centric Occlusion in The Subjects With Class Ii Div1 and Class I NormaDocument6 pages18.a Cephalometric Evaluation of Tongue From The Rest Position To Centric Occlusion in The Subjects With Class Ii Div1 and Class I NormaThendral DevanathanNo ratings yet
- Bite Force Analysis in Different Types of Angle MalocclusionsDocument12 pagesBite Force Analysis in Different Types of Angle Malocclusionsد.عاصم صويلحNo ratings yet
- Orthodontic Case History and Clinical ExaminationDocument41 pagesOrthodontic Case History and Clinical ExaminationRajesh Gyawali100% (26)
- Effects of Maxillary Protraction For Early Correction of Class IIIDocument7 pagesEffects of Maxillary Protraction For Early Correction of Class IIIMariana SantosNo ratings yet
- Treatment Planning for Loss of First Permanent MolarsDocument6 pagesTreatment Planning for Loss of First Permanent Molarsplayer osamaNo ratings yet
- Occlusal Contacts RetentionDocument9 pagesOcclusal Contacts RetentionRockey ShrivastavaNo ratings yet
- Long-Term Benefits of Early Treatment for Pseudo Class III MalocclusionDocument8 pagesLong-Term Benefits of Early Treatment for Pseudo Class III MalocclusionManena RivoltaNo ratings yet
- Mode of Action and Effects of Functional AppliancesDocument89 pagesMode of Action and Effects of Functional AppliancesSaherish FarhanNo ratings yet
- Treatment of Adults With Anterior Mandibular Teeth Crowding: Reliability of Little's Irregularity IndexDocument8 pagesTreatment of Adults With Anterior Mandibular Teeth Crowding: Reliability of Little's Irregularity IndexNaeem MoollaNo ratings yet
- Space Closure by AlmuzianDocument16 pagesSpace Closure by AlmuzianNizam MuhamadNo ratings yet
- Management of Class IIIDocument26 pagesManagement of Class IIItowncommitteeabdulhakim15401No ratings yet
- Seminar-Functional Regulator 14-08-2020Document135 pagesSeminar-Functional Regulator 14-08-2020Saumya SinghNo ratings yet
- Class II Malocclusion Treatment OptionsDocument12 pagesClass II Malocclusion Treatment OptionsPedro Dionísio LealNo ratings yet
- Fixed FunctionalDocument14 pagesFixed FunctionalsuchitraNo ratings yet
- ALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020Document3 pagesALTERNATE RAPID MAXILLARY EXPANSION AND CONSTRICTION (ALT-RAMEC) MAY BE MORE EFFECTIVE THAN RAPID MAXILLARY EXPANSION ALONE FOR PROTRACTION FACIAL MASK TREATMENTzhao2020محمد نبيل الدعيس100% (1)
- Effects of Functional Versus Bisected Occlusal Planes On The Wits AppraisalDocument5 pagesEffects of Functional Versus Bisected Occlusal Planes On The Wits AppraisalAlejandra Zambrano ValeroNo ratings yet
- Magnetic Twin BlockDocument28 pagesMagnetic Twin BlockSwapnil MangwadeNo ratings yet