You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Adhesive Cementation of Indirect Composite Inlays and Onlays: A Literature ReviewDocument9 pagesAdhesive Cementation of Indirect Composite Inlays and Onlays: A Literature ReviewAbdelrahman GalalNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- IDS ProcedureDocument7 pagesIDS ProcedurejarodzeeNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Cephalometric Outcomes of Maxillary Expansion and Protraction in PatientsDocument5 pagesCephalometric Outcomes of Maxillary Expansion and Protraction in PatientsHoang NhanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- One-Stage Closure of Isolated Cleft Palate With TheDocument8 pagesOne-Stage Closure of Isolated Cleft Palate With TheHoang NhanNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Magne IDS InstructionsDocument1 pageMagne IDS InstructionsAnonymous CY62A9No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Sequencinginpanfacialtrauma 140507004851 Phpapp02Document46 pagesSequencinginpanfacialtrauma 140507004851 Phpapp02Hoang NhanNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Analysis of Complications in Primary Cleft LipsDocument4 pagesAnalysis of Complications in Primary Cleft LipsHoang NhanNo ratings yet
- Anatomy of Maxilla and Its Development - ORIGINALDocument68 pagesAnatomy of Maxilla and Its Development - ORIGINALHoang NhanNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Cleft Lip Book EnglishDocument89 pagesCleft Lip Book Englishwerewolf3107No ratings yet
- Cắt Chóp Nạo Nang Trám NgượcDocument27 pagesCắt Chóp Nạo Nang Trám NgượcHoang NhanNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 1-Page Productivity PlannerDocument1 page1-Page Productivity PlannerLaertes105100% (5)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- TMJ PPT 130516130311 Phpapp02Document120 pagesTMJ PPT 130516130311 Phpapp02Hoang NhanNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Step 1: Formula For Calculation of Global Hunger Index ScoresDocument1 pageStep 1: Formula For Calculation of Global Hunger Index ScoresSunday FiveNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- TPN CalculationDocument3 pagesTPN CalculationSARANYANo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
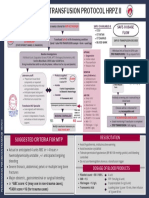
- Final Version MTP Poster 2022 2Document1 pageFinal Version MTP Poster 2022 2Hema Malini ArmugamNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Spinal Subdural Hematoma Responsible For A Syndrome of The Tail of A Horse About A Case in The University Hospital Center of Guadeloupe and Review of LiteratureDocument4 pagesSpinal Subdural Hematoma Responsible For A Syndrome of The Tail of A Horse About A Case in The University Hospital Center of Guadeloupe and Review of LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 에티오피아 제약 의료기기 인허가 절차 소개 - 영문Document39 pages에티오피아 제약 의료기기 인허가 절차 소개 - 영문Kidist TesfayeNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Borang Diabetes Clinical AuditDocument2 pagesBorang Diabetes Clinical AuditHafizzah Mohd FirdausNo ratings yet
- Midline Diastema Correction Utilizing Clinical Application of M-Spring A Case ReportDocument3 pagesMidline Diastema Correction Utilizing Clinical Application of M-Spring A Case ReportInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Activity 2 Finals Histo Lab - EDLAY2ADocument2 pagesActivity 2 Finals Histo Lab - EDLAY2ATom Anthony TonguiaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- ST Bernard GuideDocument12 pagesST Bernard GuidesuzypienaarNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- G11 HOPE Module 6Document16 pagesG11 HOPE Module 6Unk NownNo ratings yet
- PEP For NetballDocument40 pagesPEP For Netballsaiqa67% (3)
- Superficial Parotidectomy TRZDocument20 pagesSuperficial Parotidectomy TRZdokteraan100% (3)
- Full Download Reflect and Relate An Introduction To Interpersonal Communication 3rd Edition Mccornack Solutions ManualDocument24 pagesFull Download Reflect and Relate An Introduction To Interpersonal Communication 3rd Edition Mccornack Solutions Manualmauzynessa553100% (36)
- Dangerous To Go AloneDocument46 pagesDangerous To Go AlonePatrickCoxNo ratings yet
- Internship ReportDocument39 pagesInternship ReportOdongo Isaac100% (4)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Fundamentals of Occlusion Article PDFDocument6 pagesFundamentals of Occlusion Article PDFIacob Anca MihaelaNo ratings yet
- Initial AssessmentDocument27 pagesInitial Assessmentkurnia ciptaNo ratings yet
- Incident Reporting Process VisioDocument1 pageIncident Reporting Process Visiopjtx100No ratings yet
- Curs 1 ENGLEZADocument40 pagesCurs 1 ENGLEZAnistorica_iuliaNo ratings yet
- View Point 2 File 10 Teacher Leticia Franco Unit 9 1. Complete The Conversation With Whatever, Whichever, WhoeverDocument8 pagesView Point 2 File 10 Teacher Leticia Franco Unit 9 1. Complete The Conversation With Whatever, Whichever, WhoeverMaisa BassiniNo ratings yet
- MDH State Rapid Response Investigative Public Report The Waters On MayowoodDocument13 pagesMDH State Rapid Response Investigative Public Report The Waters On MayowoodinforumdocsNo ratings yet
- DR - Hawary Revision TableDocument3 pagesDR - Hawary Revision TableAseel ALshareefNo ratings yet
- Saoud 2016Document9 pagesSaoud 2016Yessica ChiuNo ratings yet
- Laboratory ManagementDocument6 pagesLaboratory ManagementJamille CarayuganNo ratings yet
- lastCleanException 20221129215815Document2 pageslastCleanException 20221129215815poisoxnedNo ratings yet
- Do Not Resuscitate in The Operating Room - Suspend or Not To SuspendDocument4 pagesDo Not Resuscitate in The Operating Room - Suspend or Not To SuspendEsteban García EcheverryNo ratings yet
- Improvement in Quality MetricsDocument10 pagesImprovement in Quality MetricsGodFather xNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Inclusive Educ PDFDocument12 pagesInclusive Educ PDFHannahNo ratings yet
- How Woud You Describe Yourself?Document5 pagesHow Woud You Describe Yourself?KC CampilanNo ratings yet
- Unit 2: MBH402 Mba 4 SemesterDocument6 pagesUnit 2: MBH402 Mba 4 SemesterSáas JainNo ratings yet