You might also like
- How To Manage Heart Failure New Guidelines 2018Document3 pagesHow To Manage Heart Failure New Guidelines 2018Dana BursacovschiNo ratings yet
- Fluids Electrolytes - Acid-Base BalanceDocument11 pagesFluids Electrolytes - Acid-Base BalanceJhosita Flora Laroco100% (1)
- Power of Vitamin D - A Vitamin D - Zaidi MD, SarfrazDocument179 pagesPower of Vitamin D - A Vitamin D - Zaidi MD, SarfrazElena DutuNo ratings yet
- Textbook Ebook Diagnostic Ultrasound For Sonographers Aya Kamaya All Chapter PDFDocument43 pagesTextbook Ebook Diagnostic Ultrasound For Sonographers Aya Kamaya All Chapter PDFolivia.anderson705100% (7)
- Proper Fluid Therapy, Vasopressors, and Inotropic - Dr. VidyaDocument40 pagesProper Fluid Therapy, Vasopressors, and Inotropic - Dr. VidyaTinton PristiantoNo ratings yet
- Diagnosis of Heart Failure With Preserved Ejection FractionDocument8 pagesDiagnosis of Heart Failure With Preserved Ejection FractionErwin GuerreroNo ratings yet
- Clinical Assessment in Acute Heart Failure: Review ArticleDocument17 pagesClinical Assessment in Acute Heart Failure: Review ArticleAnonymous NeRC5JYiSNo ratings yet
- Brahmbhatt 2018Document7 pagesBrahmbhatt 2018Jr SparkNo ratings yet
- Heart Failure With Preserved Ejection Fraction HF PEF A Mini ReviewDocument3 pagesHeart Failure With Preserved Ejection Fraction HF PEF A Mini ReviewPaul HartingNo ratings yet
- Heart Failure in Sub-Saharan Africa: A Clinical Approach: ReviewDocument9 pagesHeart Failure in Sub-Saharan Africa: A Clinical Approach: ReviewrizkaNo ratings yet
- Congestive Heart FailureDocument13 pagesCongestive Heart FailureAgeng BudianantiNo ratings yet
- DR - TrisuloDocument35 pagesDR - TrisuloZaky prasetyaNo ratings yet
- Study of The Role of Plasma Nt-Probnp in The Diagnosis of Heart FailureDocument5 pagesStudy of The Role of Plasma Nt-Probnp in The Diagnosis of Heart FailureMinerva Medical Treatment Pvt LtdNo ratings yet
- Echocardiography in Heart Failure: A Guide For General PracticeDocument6 pagesEchocardiography in Heart Failure: A Guide For General PracticesavitageraNo ratings yet
- Heart Failure - ReferatDocument10 pagesHeart Failure - ReferatAlbert ShantoNo ratings yet
- Heart FailureDocument8 pagesHeart FailureKKUTC PerlisNo ratings yet
- Heart Failure With Normal Ejection Fraction (HFNEF) : Is It Worth Considering?Document7 pagesHeart Failure With Normal Ejection Fraction (HFNEF) : Is It Worth Considering?bhaskarpurushottamNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument7 pagesHeart Failure With Preserved Ejection FractionJoko NahamaNo ratings yet
- Atrial Fibrillation (AF) & Flutter Complicating Critical IllnessDocument29 pagesAtrial Fibrillation (AF) & Flutter Complicating Critical IllnessMohammed SadoonNo ratings yet
- Ehw128 AddendaDocument6 pagesEhw128 AddendaClement ThansNo ratings yet
- Congestive Heart Failure: Dr. Asif WazirDocument21 pagesCongestive Heart Failure: Dr. Asif WazirHillary BushnellNo ratings yet
- Ghid Heart FailureDocument117 pagesGhid Heart FailureIlie RoxanaNo ratings yet
- 2016 ESC Guidelines For The Diagnosis and TreatmentDocument52 pages2016 ESC Guidelines For The Diagnosis and TreatmentDedy KristoferNo ratings yet
- 67-Article Text-115-1-10-20171026Document5 pages67-Article Text-115-1-10-20171026Maria MiripNo ratings yet
- Clinical Definition of Heart FailureDocument12 pagesClinical Definition of Heart FailureFreddy PanjaitanNo ratings yet
- Jeab 154Document28 pagesJeab 154Yilianeth MenaNo ratings yet
- Case Study On Congestive Heart FailureDocument5 pagesCase Study On Congestive Heart Failureaxmedfare138No ratings yet
- Insuficiencia Cardiaca Neyssa KimeeDocument33 pagesInsuficiencia Cardiaca Neyssa KimeeNEYSSA KIMEE SAINT VILNo ratings yet
- Systolic Vs Diastolic Heart FailureDocument57 pagesSystolic Vs Diastolic Heart FailureRashiden MadjalesNo ratings yet
- Cme HFDocument30 pagesCme HFTze SiangNo ratings yet
- Congestive Heart FailureDocument25 pagesCongestive Heart Failuredexter veracityNo ratings yet
- Dirk L. Brutsaert 2007-1Document9 pagesDirk L. Brutsaert 2007-1CARLOS FRANCISCO MANTILLA MONTALVONo ratings yet
- PTR 26 01Document9 pagesPTR 26 01Langit BiruNo ratings yet
- Investigation and Management of Congestive Heart Failure: Clinical ReviewDocument6 pagesInvestigation and Management of Congestive Heart Failure: Clinical ReviewDwiky YuanasikaNo ratings yet
- Clinical Epidemiology of Heart Failure: Arend Mosterd, Arno W HoesDocument11 pagesClinical Epidemiology of Heart Failure: Arend Mosterd, Arno W HoesCAMILO ANDRES TOVAR DAZANo ratings yet
- Garcia 2016 Constrictive Pericarditis Versus Restrictive CardiomyopathyDocument16 pagesGarcia 2016 Constrictive Pericarditis Versus Restrictive CardiomyopathysunprizeproductionNo ratings yet
- Heart Failure With Preserved Ejection Fraction (Hfpef) : A Basic and Clinical PerspectiveDocument5 pagesHeart Failure With Preserved Ejection Fraction (Hfpef) : A Basic and Clinical PerspectiveOngky AristianNo ratings yet
- Current Status of Heart Failure Reduce EF Management, All at Once-2Document29 pagesCurrent Status of Heart Failure Reduce EF Management, All at Once-2Sasmita DewiNo ratings yet
- Penanganan Gagal Jantung Diastolik: Starry H. RampenganDocument9 pagesPenanganan Gagal Jantung Diastolik: Starry H. Rampenganpaul silabanNo ratings yet
- Innovation in Clinical Care in Heart FailureDocument107 pagesInnovation in Clinical Care in Heart FailureSebastian Henao ErazoNo ratings yet
- 10 1002@ejhf 1858Document15 pages10 1002@ejhf 1858HnWishNo ratings yet
- Cardiac FailureDocument7 pagesCardiac FailureCasuga, Jessica Carmela F.No ratings yet
- Acute Lung Edema Management PracticeDocument5 pagesAcute Lung Edema Management PracticeYunia DuanaNo ratings yet
- Heart Failure With Preserved Ejection Fraction: Authors: Andrew R HarperDocument6 pagesHeart Failure With Preserved Ejection Fraction: Authors: Andrew R HarperOngky AristianNo ratings yet
- De Novo Acute Heart Failure and Acutely Decompensated Chronic Heart Failure PDFDocument14 pagesDe Novo Acute Heart Failure and Acutely Decompensated Chronic Heart Failure PDFEffika PutriNo ratings yet
- 1414 431X BJMBR 53 7 E9646Document16 pages1414 431X BJMBR 53 7 E9646leidyalexserraoNo ratings yet
- Incidence Pathophysiology Classification Causes Diagnosis Assessing Cardiovascular Disability Treatment MessagesDocument67 pagesIncidence Pathophysiology Classification Causes Diagnosis Assessing Cardiovascular Disability Treatment MessagesAhmed ElshewiNo ratings yet
- Heart Failure: Clinical Manifestations and Diagnosis in Adults - UpToDateDocument44 pagesHeart Failure: Clinical Manifestations and Diagnosis in Adults - UpToDateJulia Pelissaro CarboniNo ratings yet
- The Difference Between Pulmonary Hypertension and Pulmonary EmboliDocument79 pagesThe Difference Between Pulmonary Hypertension and Pulmonary EmboliRizqon RohmatussadeliNo ratings yet
- Manejo Falla Cardiaca Aguda en Gatos PDFDocument17 pagesManejo Falla Cardiaca Aguda en Gatos PDFFelipeNo ratings yet
- 1 A 07 051-062 Unlocked PDFDocument11 pages1 A 07 051-062 Unlocked PDFHarest FauziNo ratings yet
- Físico Patología Falla CardiacaDocument19 pagesFísico Patología Falla CardiacavictorNo ratings yet
- Acute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihaDocument98 pagesAcute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihablackcatNo ratings yet
- Circheartfailure 114 001100Document9 pagesCircheartfailure 114 001100graldNo ratings yet
- Heart Failure OlderDocument18 pagesHeart Failure OlderRESIDENTES MEDICINA INTERNANo ratings yet
- Heart FailureDocument80 pagesHeart Failuregalemayehu471No ratings yet
- I. Acute Heart Failure: What Every Physician Needs To KnowDocument13 pagesI. Acute Heart Failure: What Every Physician Needs To KnowRubie Ann TillorNo ratings yet
- HFpEF Management 2023Document10 pagesHFpEF Management 2023ctsakalakisNo ratings yet
- Congestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareDocument10 pagesCongestive Heart Failure: Diagnosis, Pathophysiology, Therapy, and Implications For Respiratory CareMirachel AugustNo ratings yet
- Chronic Heart Failure CHFDocument11 pagesChronic Heart Failure CHFChen BrionesNo ratings yet
- THROMBOSISDocument11 pagesTHROMBOSISChandan DebbarmaNo ratings yet
- Ghost CapDocument4 pagesGhost Capmedico89No ratings yet
- Nursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)Document35 pagesNursing Management of Criticallyill Patient: Prepared By: Ms Mononita Bhattacharjee (M.SC Medical Surgical Nursing)priyagerardNo ratings yet
- A (ACLS) - 2015: Dvanced Cardiac Life SupportDocument52 pagesA (ACLS) - 2015: Dvanced Cardiac Life SupportNajmussaqibNo ratings yet
- Delirium and DementiaDocument12 pagesDelirium and DementiaSNo ratings yet
- BlocK J 2023 Paper KGMCDocument27 pagesBlocK J 2023 Paper KGMCsafat ullah50No ratings yet
- Diseases Associated With The Various Organ SystemsDocument10 pagesDiseases Associated With The Various Organ SystemsKimh SampagNo ratings yet
- 11 Lung PathologyDocument7 pages11 Lung PathologycarlgangcaNo ratings yet
- Dyspneabyahammednaseem 210628024048Document19 pagesDyspneabyahammednaseem 210628024048Naseem Bin YoosafNo ratings yet
- Oxo AQAGCSE B7 ws01 XxaannDocument2 pagesOxo AQAGCSE B7 ws01 XxaannParam BhimaniNo ratings yet
- The Complete Revision Guide For The FRCR Exam Revised 3-64986Document48 pagesThe Complete Revision Guide For The FRCR Exam Revised 3-64986Benjamin Barsouma MathewNo ratings yet
- Chest Pain Algorithm Clinical Case Scenarios PDF 243970669Document28 pagesChest Pain Algorithm Clinical Case Scenarios PDF 243970669Romelu MartialNo ratings yet
- PDF First Aid For The Pediatrics Clerkship 4E True 4Th Edition Latha Ganti Ebook Full ChapterDocument53 pagesPDF First Aid For The Pediatrics Clerkship 4E True 4Th Edition Latha Ganti Ebook Full Chapterjohnathan.cucuzza496100% (1)
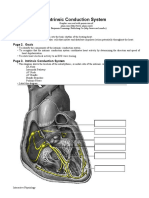
- Intrinsic Conduction System: Page 1. IntroductionDocument5 pagesIntrinsic Conduction System: Page 1. IntroductionUta Provinsiana SukmaraNo ratings yet
- 10 Besar Penyakit 2021Document14 pages10 Besar Penyakit 2021Elisa MathildaNo ratings yet
- Diseases of The Peripheral Nervous System - PDFXDocument122 pagesDiseases of The Peripheral Nervous System - PDFXShams JailaniNo ratings yet
- Wa0016.Document176 pagesWa0016.Sreeja ReddyNo ratings yet
- Komplikasi DM: Hemi SinoritaDocument26 pagesKomplikasi DM: Hemi SinoritaPapah ZiyanNo ratings yet
- SLE SketchyDocument2 pagesSLE SketchyLanaAmerieNo ratings yet
- Diltiazem Hydro ChlorideDocument3 pagesDiltiazem Hydro Chlorideapi-3797941100% (1)
- Ear LesionsDocument4 pagesEar LesionsJose SirittNo ratings yet
- Tematica Licenta 2012 2013 FMF Oradea Medicina in Limba EnglezaDocument3 pagesTematica Licenta 2012 2013 FMF Oradea Medicina in Limba EnglezaLacramioara_Te_3375No ratings yet
- Development and Validation of A Preoperative Scoring System To Predict 30 Day Mortality in Patients Undergoing Hip Fracture SurgeryDocument7 pagesDevelopment and Validation of A Preoperative Scoring System To Predict 30 Day Mortality in Patients Undergoing Hip Fracture Surgeryuhs888No ratings yet
- Gastroenterology PancreatitisDocument1 pageGastroenterology PancreatitisNour SamadNo ratings yet
- Pegasus TIMI 54 TrialDocument13 pagesPegasus TIMI 54 TrialIsaac Aaron Enriquez MonsalvoNo ratings yet
- COP 8 ICU Manual - docx-PANCHAMDocument16 pagesCOP 8 ICU Manual - docx-PANCHAMSumit SardanaNo ratings yet
- CIED Surgical Guidance Dec21Document16 pagesCIED Surgical Guidance Dec21SamNo ratings yet