You might also like
- Human Gene TherapyDocument18 pagesHuman Gene TherapyAnupriya SinghNo ratings yet
- PMDC NEB Exam Medical FormatDocument6 pagesPMDC NEB Exam Medical FormatShawn Parker57% (7)
- Gene Therapy1Document40 pagesGene Therapy1Sindhu SmileyNo ratings yet
- Bacteria Vs Viruses PPT 2019Document25 pagesBacteria Vs Viruses PPT 2019Rene Ramilo100% (1)
- Cervical Cancer: Dr. Sushma DhakalDocument137 pagesCervical Cancer: Dr. Sushma DhakalBhattarai ShrinkhalaNo ratings yet
- Manual of Diagnostic Antibodies For Immunohistology - 1841101001Document539 pagesManual of Diagnostic Antibodies For Immunohistology - 1841101001dudapaskasNo ratings yet
- Gene Therapy: Hereditary or Acquired Genetic DefectsDocument66 pagesGene Therapy: Hereditary or Acquired Genetic DefectsDRx Sonali TareiNo ratings yet
- Gene TherapyDocument25 pagesGene TherapynooNo ratings yet
- Gene TherapyDocument20 pagesGene TherapyHugo SantanaNo ratings yet
- Gene Therapy: Its Applications &Document39 pagesGene Therapy: Its Applications &Rose DeymNo ratings yet
- Gene Therapy: By: Lucila Odelan C. MercadoDocument33 pagesGene Therapy: By: Lucila Odelan C. MercadoLj Paul YumulNo ratings yet
- NP2 Nursing Board Exam November 2008Document16 pagesNP2 Nursing Board Exam November 2008Clarissa GuifayaNo ratings yet
- L - 10 Gene TherapyDocument6 pagesL - 10 Gene TherapyDimple CobachaNo ratings yet
- Weather Climate NotesDocument61 pagesWeather Climate NotesRene Ramilo100% (1)
- Business FinanceDocument340 pagesBusiness FinanceRene Ramilo83% (6)
- Gene TherapyDocument40 pagesGene TherapyMahbubul Islam Koushick100% (1)
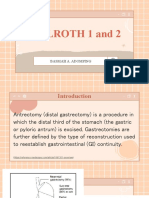
- Billroth 1 and 2: Basmah A. AdompingDocument31 pagesBillroth 1 and 2: Basmah A. AdompingBasmah A. AdompingNo ratings yet
- Gene Therapy: Course InstructorDocument28 pagesGene Therapy: Course InstructorSamiul Alam RajibNo ratings yet
- Gene Therapy 1Document25 pagesGene Therapy 1Shobha RangappaNo ratings yet
- English For NursingDocument30 pagesEnglish For NursingKiki SeptyantiNo ratings yet
- GEOTHERMAL ENERGY PowerPointDocument25 pagesGEOTHERMAL ENERGY PowerPointRene RamiloNo ratings yet
- IM Written Report Diabetes Case ReportDocument10 pagesIM Written Report Diabetes Case ReportJessa Mateum VallangcaNo ratings yet
- 28 Biochemic CombinationDocument6 pages28 Biochemic CombinationMustafa AliNo ratings yet
- Gene Therapi PDFDocument56 pagesGene Therapi PDFbhargav patelNo ratings yet
- Gene TherapyDocument7 pagesGene Therapydarlene consignado100% (1)
- Gene Therapy: Strategies and Clinical ApplicationsDocument44 pagesGene Therapy: Strategies and Clinical ApplicationsjeorajaNo ratings yet
- Gene Therapy Final-1Document45 pagesGene Therapy Final-1Navpreet KaurNo ratings yet
- Unit 1 Gene Therapy - Introduction PDFDocument98 pagesUnit 1 Gene Therapy - Introduction PDFbalanashish774No ratings yet
- GeneDocument56 pagesGeneACTION plusNo ratings yet
- Gene Therapy FinalDocument43 pagesGene Therapy FinalGlory NeriNo ratings yet
- Biology - Kashvi - Gene TherapyDocument56 pagesBiology - Kashvi - Gene TherapyKashvi ShriNo ratings yet
- Gene Therapy1Document26 pagesGene Therapy1fangekeNo ratings yet
- Gene Therapy1Document37 pagesGene Therapy1rajnishsunil5No ratings yet
- Gene Therapy: September 14 1990 U.S. National Institutes of Health W. French AndersonDocument20 pagesGene Therapy: September 14 1990 U.S. National Institutes of Health W. French AndersonSamatha MohanNo ratings yet
- Gene Therapy 1Document22 pagesGene Therapy 1Priya ChaudharyNo ratings yet
- Gene Therapy Main 160215021217Document56 pagesGene Therapy Main 160215021217wooodsfrank21No ratings yet
- Gene TherapyDocument9 pagesGene TherapySumaNo ratings yet
- Gene TherapyDocument7 pagesGene TherapyMerrylFranciscoNo ratings yet
- The Aspects of Gene TherapyDocument9 pagesThe Aspects of Gene TherapyCharice Anne VillamarinNo ratings yet
- Gene TherapyDocument7 pagesGene TherapySaba RiazNo ratings yet
- Gene TherapyDocument29 pagesGene Therapynabeel nadeemNo ratings yet
- STS - Stem Cell TherapyDocument29 pagesSTS - Stem Cell TherapyMec AmilasanNo ratings yet
- Z (H) IV GE Animal Cell BiotechnologyDocument59 pagesZ (H) IV GE Animal Cell BiotechnologySudeshna ChakrabortyNo ratings yet
- Unit-4 GENE THERAPYDocument65 pagesUnit-4 GENE THERAPYPratanu KayetNo ratings yet
- Aspects of Gene Therapy Group 5 1Document16 pagesAspects of Gene Therapy Group 5 1geline21No ratings yet
- Treatment For Genetic Disorders Using Techniques That Replace or Supplement The Defective GeneDocument19 pagesTreatment For Genetic Disorders Using Techniques That Replace or Supplement The Defective Geneapi-26229242No ratings yet
- Terapi GenDocument81 pagesTerapi Genyudha fahmiNo ratings yet
- Gene Therapy - Arpita MishraDocument26 pagesGene Therapy - Arpita MishraBiotech PressNo ratings yet
- Stem Cell Gene TherapyDocument2 pagesStem Cell Gene TherapyJuderussell GarciaNo ratings yet
- Biotechnology in HealthDocument5 pagesBiotechnology in HealthInea GambalanNo ratings yet
- Soroori-Motlagh Nastaran 200705 (SCID)Document29 pagesSoroori-Motlagh Nastaran 200705 (SCID)Charles IppolitoNo ratings yet
- Gene Therapy AND Human Genome Project: DR - Vidya.S.Patil Prof and Head Dept of Biochemistry SDMCMS &H, DharwadDocument23 pagesGene Therapy AND Human Genome Project: DR - Vidya.S.Patil Prof and Head Dept of Biochemistry SDMCMS &H, DharwadStarboy NeillNo ratings yet
- Gene TherapyDocument19 pagesGene TherapySmyle KatariaNo ratings yet
- Gene TherapyDocument30 pagesGene TherapypklarenzanneNo ratings yet
- Presentation: Gene Therapy!! Presented By: Nitish Pathania Sec: Re7802a03 Reg - Id 10803694Document34 pagesPresentation: Gene Therapy!! Presented By: Nitish Pathania Sec: Re7802a03 Reg - Id 10803694nitishpathaniaNo ratings yet
- Correcting Defective Genes: Gene TherapyDocument19 pagesCorrecting Defective Genes: Gene TherapyDivya VermaNo ratings yet
- Gene TherapyDocument74 pagesGene TherapyNitesh RohatgiNo ratings yet
- Human Gene Therapy: Related PapersDocument8 pagesHuman Gene Therapy: Related PapersLordsam B. ListonNo ratings yet
- Gene Therapy: Group 5Document25 pagesGene Therapy: Group 5Elisha Gwyn JadormeoNo ratings yet
- Human Gene Therapy: A Brief Overview of The Genetic RevolutionDocument7 pagesHuman Gene Therapy: A Brief Overview of The Genetic RevolutionDinda Wanodya SNo ratings yet
- Group 8 STS - Gene TheraphyDocument35 pagesGroup 8 STS - Gene TheraphyArsenio RojoNo ratings yet
- Genetic Variation and Role in Pharmacology: Presented byDocument27 pagesGenetic Variation and Role in Pharmacology: Presented byHannah EspigaNo ratings yet
- Human Gene TherapyDocument7 pagesHuman Gene Therapymichelleannmaguigad28No ratings yet
- Gene Therapy: Science, Technology & SocietyDocument25 pagesGene Therapy: Science, Technology & SocietyNicki Lyn Dela CruzNo ratings yet
- Wa0001Document14 pagesWa0001Hema ChandrikaNo ratings yet
- Gene Therapy 1Document25 pagesGene Therapy 1Casey MerencilloNo ratings yet
- Geene TherapyDocument24 pagesGeene TherapyAwais GulNo ratings yet
- L19 DNAtech Rev Genetics 2013 FDocument27 pagesL19 DNAtech Rev Genetics 2013 FjdazuelosNo ratings yet
- Rekayasa Genetik Dan Terapi Gen: Bagian Biokimia Fakultas Kedokteran Universitas Hasanuddin MakassarDocument36 pagesRekayasa Genetik Dan Terapi Gen: Bagian Biokimia Fakultas Kedokteran Universitas Hasanuddin MakassarHenny Taufik GosalNo ratings yet
- Module 7 - Infectious DiseaseDocument50 pagesModule 7 - Infectious Diseaseshwetlana rampureNo ratings yet
- Xenotransplantation: Current Issues of XenotransplantationDocument3 pagesXenotransplantation: Current Issues of Xenotransplantationfreemens1No ratings yet
- A Compilation of Cellular and Tissue Xenotransplantation Studies (1838-2022): A Promising Approach for the Treatment of DiseasesFrom EverandA Compilation of Cellular and Tissue Xenotransplantation Studies (1838-2022): A Promising Approach for the Treatment of DiseasesNo ratings yet
- Laboratory Activity BIOLOGY 07-08Document24 pagesLaboratory Activity BIOLOGY 07-08Rene RamiloNo ratings yet
- Macmeyers ActivityDocument28 pagesMacmeyers ActivityRene RamiloNo ratings yet
- Psychological Understanding of The Emerging Technological DriftDocument29 pagesPsychological Understanding of The Emerging Technological DriftRene RamiloNo ratings yet
- EGG SHELL As Acid NeutralizerDocument9 pagesEGG SHELL As Acid NeutralizerRene RamiloNo ratings yet
- Why Use Technology in Science ClassroomDocument15 pagesWhy Use Technology in Science ClassroomRene RamiloNo ratings yet
- Semana UCLADocument7 pagesSemana UCLAAndre BanhateNo ratings yet
- Pharmacotherapy of StrokeDocument37 pagesPharmacotherapy of StrokeAndykaYayanSetiawanNo ratings yet
- Science - December 14, 2018 USA PDFDocument203 pagesScience - December 14, 2018 USA PDFdariaNo ratings yet
- Back To Nature Reading & WritingDocument23 pagesBack To Nature Reading & Writingmaiche amarNo ratings yet
- Diagnostic Report: Patient Name: Razia Sultana FH.11964170 0026VI003012Document2 pagesDiagnostic Report: Patient Name: Razia Sultana FH.11964170 0026VI003012Zeeshan QureshiNo ratings yet
- Urology Case Report 2Document2 pagesUrology Case Report 2rachana gargNo ratings yet
- The Thaakat Insider - Summer 2012 EditionDocument4 pagesThe Thaakat Insider - Summer 2012 EditionthaakatNo ratings yet
- NCM 102 PDFDocument8 pagesNCM 102 PDFjnnfrleeeNo ratings yet
- Cytotoxic PrecautionsDocument27 pagesCytotoxic Precautionsstephanie wilcoxNo ratings yet
- Journal: European RespiratoryDocument3 pagesJournal: European RespiratoryMercy HasanNo ratings yet
- Edema of The Uvula: Etiology, Risk Factors, Diagnosis, and TreatmentDocument4 pagesEdema of The Uvula: Etiology, Risk Factors, Diagnosis, and TreatmentAfri AdiNo ratings yet
- NGT PresentationDocument23 pagesNGT PresentationniyigokNo ratings yet
- CHOLELITHIASISSDocument29 pagesCHOLELITHIASISSAngelica Mercado SirotNo ratings yet
- Gall Bladder - : Anatomy, Physiology and Benign Disease For Medical UndergraduatesDocument119 pagesGall Bladder - : Anatomy, Physiology and Benign Disease For Medical UndergraduatesMayadevi100% (1)
- Impact of Male Circumcision in ChitungwizaDocument76 pagesImpact of Male Circumcision in ChitungwizaChristian Kusema Jr.No ratings yet
- OSTEOSARCOMA: A Literature Review and Case StudyDocument12 pagesOSTEOSARCOMA: A Literature Review and Case StudySyarafina NadilaNo ratings yet
- Practice Essentials of Pulmonary ThromboembolismDocument39 pagesPractice Essentials of Pulmonary ThromboembolismEzzat Abdelhafeez SalemNo ratings yet
- Otolaryngology Privileges PDFDocument11 pagesOtolaryngology Privileges PDFAzwar RidhwanNo ratings yet
- 9 Wjuu 1338452328Document12 pages9 Wjuu 1338452328Codecom SisgeNo ratings yet
- Thyroid Dse - SupersummaryDocument3 pagesThyroid Dse - SupersummaryMissDyYournurseNo ratings yet
- 4 PutterDocument57 pages4 PutterFilip IonescuNo ratings yet
- Pharmacogenomics PDFDocument12 pagesPharmacogenomics PDFsivaNo ratings yet