You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- OPENING Speak As PICDocument1 pageOPENING Speak As PICshellyzukhraNo ratings yet
- AFP (alpha-fetoprotein) as a marker for hepatocellular carcinomaDocument19 pagesAFP (alpha-fetoprotein) as a marker for hepatocellular carcinomashellyzukhraNo ratings yet
- ISGO 2017 - 1st AnnouncementDocument3 pagesISGO 2017 - 1st AnnouncementshellyzukhraNo ratings yet
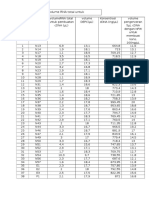
- Lampiran 4 .Jumlah Volume RNA Total Untuk Pembuatan cDNADocument2 pagesLampiran 4 .Jumlah Volume RNA Total Untuk Pembuatan cDNAshellyzukhraNo ratings yet
- Fialova PAPPADocument12 pagesFialova PAPPAshellyzukhraNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Doulas of South Australia - Qualified and Trainee DoulasDocument2 pagesDoulas of South Australia - Qualified and Trainee DoulasHelenRomeoNo ratings yet
- Effectiveness of Structured Teaching Programme On Knowledge Regarding The Breast Engorgement Among Postnatal Mother With Breast EngorgementDocument2 pagesEffectiveness of Structured Teaching Programme On Knowledge Regarding The Breast Engorgement Among Postnatal Mother With Breast EngorgementIJAR JOURNALNo ratings yet
- NOBEL Group 1 Handout TDocument5 pagesNOBEL Group 1 Handout TAdrian GabrielNo ratings yet
- Nahata, Chen, Moravek, Quinn, Sutter, Taylor, Tishelman, & Gomez-Lobo, 2019Document7 pagesNahata, Chen, Moravek, Quinn, Sutter, Taylor, Tishelman, & Gomez-Lobo, 2019Anonymous 75M6uB3OwNo ratings yet
- CHAPTER 2 Unpacking The SelfDocument28 pagesCHAPTER 2 Unpacking The SelfRachelle Salcedo82% (11)
- HPV Lesson Plan PDFDocument25 pagesHPV Lesson Plan PDFMonique MavronicolasNo ratings yet
- Factors Affecting LaborDocument2 pagesFactors Affecting LaborChristina Richards100% (1)
- Polycystic Ovary SyndromeDocument11 pagesPolycystic Ovary SyndromeABC11No ratings yet
- Case Study H MOLEDocument11 pagesCase Study H MOLEmaori_martinez82% (11)
- NCPFORMATstudentcopy 2Document4 pagesNCPFORMATstudentcopy 2Reinhardt MostolesNo ratings yet
- B1 2 Coordination & Control Questions and AnswersDocument36 pagesB1 2 Coordination & Control Questions and AnswersBioScMentor-1No ratings yet
- Abortion PP TDocument42 pagesAbortion PP TDivya ToppoNo ratings yet
- Menopause Daftar PustakaDocument3 pagesMenopause Daftar PustakaMuhammad Izzuddin Abdul JalilNo ratings yet
- Homework Assignment 4Document3 pagesHomework Assignment 4azoric21850% (2)
- اختصارات المندوه ObstetricsDocument11 pagesاختصارات المندوه ObstetricssamyNo ratings yet
- The National Birth Center Study IIDocument12 pagesThe National Birth Center Study IIapi-38108107No ratings yet
- Fetal risks of macrosomia in diabetic pregnanciesDocument27 pagesFetal risks of macrosomia in diabetic pregnanciesIful SaifullahNo ratings yet
- Kinship, Marriage, Family and Household StructuresDocument3 pagesKinship, Marriage, Family and Household StructuresAr Anne Ugot60% (10)
- OBG AbbreviationsDocument36 pagesOBG AbbreviationsSivakumarNo ratings yet
- Management of Rape VictimsDocument21 pagesManagement of Rape VictimsAndreea Ioana BogdanNo ratings yet
- Sex selective abortion threat to Indian womenDocument3 pagesSex selective abortion threat to Indian womentatevijayNo ratings yet
- Victims of Domestic Violence: Attacked by Husbands, Trapped by SocietyDocument5 pagesVictims of Domestic Violence: Attacked by Husbands, Trapped by Societyfhey davidNo ratings yet
- Pregnancy Assessment Health History ROSDocument34 pagesPregnancy Assessment Health History ROSteuuuuNo ratings yet
- Female Genitourinary Anatomy and FunctionDocument13 pagesFemale Genitourinary Anatomy and FunctionAnnetta AronovaNo ratings yet
- Gender Discrimination in India: An AnalysisDocument11 pagesGender Discrimination in India: An AnalysisRaja RajhansNo ratings yet
- EMBRYOLOGYDocument4 pagesEMBRYOLOGYbhagavan prasadNo ratings yet
- NURS 6551 Final ExamDocument10 pagesNURS 6551 Final ExamtroillerdrippyNo ratings yet
- Blighted Ovum PDFDocument4 pagesBlighted Ovum PDFGopurS100% (1)
- Human Sexuality CSL650 Reaction PaperDocument9 pagesHuman Sexuality CSL650 Reaction PaperTe-Erika50% (2)