You might also like
- Sabiston Textbook of Surgery 17th Ed 2005Document2,477 pagesSabiston Textbook of Surgery 17th Ed 2005Kyo Kusanagy33% (12)
- Pre-Op Case Protocol #4Document2 pagesPre-Op Case Protocol #4IC BNo ratings yet
- Rite BlueprintDocument11 pagesRite BlueprintTal Lagura100% (1)
- Chronic Liver DiseaseDocument30 pagesChronic Liver Diseaseprajwal86% (7)
- Roru Exoendo - PancreasDocument13 pagesRoru Exoendo - PancreasRitz CelsoNo ratings yet
- Case Presentation: NeurologyDocument19 pagesCase Presentation: NeurologySydrex SarmientoNo ratings yet
- Migs (With Summary) +paoDocument6 pagesMigs (With Summary) +paoMigs MedinaNo ratings yet
- Clinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzDocument31 pagesClinical Therapeutics Oral Revalida Review Notes: CASE 1: Dr. Abraham Daniel C. CruzNoreenNo ratings yet
- Difficulty Breathing Case ReportDocument6 pagesDifficulty Breathing Case ReportRaian SuyuNo ratings yet
- Osce Cranial Nerves PDFDocument42 pagesOsce Cranial Nerves PDFriczen vilaNo ratings yet
- Topnotch Practice Exam 1 For MARCH 2020 and SEPT 2020 BatchesDocument104 pagesTopnotch Practice Exam 1 For MARCH 2020 and SEPT 2020 BatchesJerome AndresNo ratings yet
- UST Medicine I Schedule 2016-2017Document6 pagesUST Medicine I Schedule 2016-2017ina17_eaglerNo ratings yet
- MBR 2019 - Physiology Handouts PDFDocument121 pagesMBR 2019 - Physiology Handouts PDFKenneth T. NuñezNo ratings yet
- SLU School of Medicine Report on PEM CasesDocument10 pagesSLU School of Medicine Report on PEM CasesJeffrey RamosNo ratings yet
- Histologic findings in mandibular mass reveal ameloblastomaDocument65 pagesHistologic findings in mandibular mass reveal ameloblastomaWilliam Tan CebrianNo ratings yet
- Medicine OB History and PE TemplateDocument9 pagesMedicine OB History and PE TemplateJanella SuerteNo ratings yet
- Final Coaching 2023Document3 pagesFinal Coaching 2023Parasaubang ButangNo ratings yet
- 2016 CPG Ent PDFDocument21 pages2016 CPG Ent PDFCamelle CelisNo ratings yet
- Legal Medicine and Medical Jurisprudence Comprehensive Exam ReviewerDocument17 pagesLegal Medicine and Medical Jurisprudence Comprehensive Exam ReviewerYeshua Tura100% (1)
- TOPNOTCH Diagnostic Exam ANSWER KEY September 2018Document20 pagesTOPNOTCH Diagnostic Exam ANSWER KEY September 2018CDNo ratings yet
- Pharmacology Table - GonzalesDocument14 pagesPharmacology Table - GonzalesMark Angelo PonferradoNo ratings yet
- The PFC MatrixDocument1 pageThe PFC MatrixAd AstraNo ratings yet
- OSCE ReviewerDocument11 pagesOSCE ReviewerJason MirasolNo ratings yet
- MBR 2019 - Radiology Handouts-Unlocked PDFDocument5 pagesMBR 2019 - Radiology Handouts-Unlocked PDFCoy EnNo ratings yet
- Renal Lab Tests ExplainedDocument67 pagesRenal Lab Tests ExplainedRjDNo ratings yet
- Final Coaching - Biochem 2022Document6 pagesFinal Coaching - Biochem 2022Jhon Paulo100% (1)
- Histology: Ust Faculty of Medicine and Surgery Class of 2016Document14 pagesHistology: Ust Faculty of Medicine and Surgery Class of 2016Ashley Beatriz PascualNo ratings yet
- Mucinous Cystadenoma 0708Document12 pagesMucinous Cystadenoma 0708eosfieldNo ratings yet
- IM Revalida Review 2019Document75 pagesIM Revalida Review 2019Nathaniel CamangonNo ratings yet
- Final Coaching - Im 2022Document9 pagesFinal Coaching - Im 2022Jhon PauloNo ratings yet
- Anesth BarashDocument6 pagesAnesth BarashIAN GABRIELLE MERCADO CUYNONo ratings yet
- EBM Self Instructional Manual 2008Document127 pagesEBM Self Instructional Manual 2008Adrian Oscar Z. Bacena100% (2)
- The "Most Common" . According To NelsonDocument31 pagesThe "Most Common" . According To NelsonKenneth NuñezNo ratings yet
- Reviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixDocument10 pagesReviewer For Pedia Osce: 10.5 KG 45.16 CM / 17.8 in 75 CM SixJamora ManilynNo ratings yet
- Clinical Practice Guidelines: Chronic Suppurative Otitis Media in AdultsDocument28 pagesClinical Practice Guidelines: Chronic Suppurative Otitis Media in Adultsnanu-jenuNo ratings yet
- Character Hypertrophic Scar Keloid: Nutshell Series For FMGE/DNB/NEET-PG-General SurgeryDocument26 pagesCharacter Hypertrophic Scar Keloid: Nutshell Series For FMGE/DNB/NEET-PG-General SurgeryAbdalsalaam AbraikNo ratings yet
- Mock PharmDocument11 pagesMock PharmLj VenethNo ratings yet
- Physio Ob ReviewDocument368 pagesPhysio Ob ReviewMark LopezNo ratings yet
- Topnotch Waiver Oath and Checklist April 2015 PDFDocument2 pagesTopnotch Waiver Oath and Checklist April 2015 PDFRalph JuicoNo ratings yet
- 01 Physiology PLE 2019 Ratio1Document62 pages01 Physiology PLE 2019 Ratio1Patricia VillegasNo ratings yet
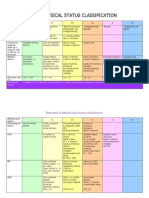
- ASA physical status classification guideDocument3 pagesASA physical status classification guideMelisa Malik0% (1)
- Tonsillopharyngitis and Obstructive Adenoidal Hypertrophy, Acute and ChronicDocument10 pagesTonsillopharyngitis and Obstructive Adenoidal Hypertrophy, Acute and ChronicHazel Fernandez VillarNo ratings yet
- January 11 January 25 February 6 February 22: Date SubjectsDocument3 pagesJanuary 11 January 25 February 6 February 22: Date SubjectsShams JailaniNo ratings yet
- Bronchial Asthma: West Visayas State University Medical Center - Department of PediatricsDocument9 pagesBronchial Asthma: West Visayas State University Medical Center - Department of PediatricsPGI Miayo, StephenNo ratings yet
- Oncologic Emergencies Management GuideDocument5 pagesOncologic Emergencies Management GuideAra DiocosNo ratings yet
- Esophageal Achalasia DysphagiaDocument14 pagesEsophageal Achalasia DysphagiaTirtha Taposh100% (1)
- March 2022 Hybrid Full Course OFFICIAL Lecture Schedule - NOV-DEC UPLOADDocument3 pagesMarch 2022 Hybrid Full Course OFFICIAL Lecture Schedule - NOV-DEC UPLOADJhon PauloNo ratings yet
- Pharmacology Finals ReviewDocument2 pagesPharmacology Finals ReviewVince CabahugNo ratings yet
- TOPNOTCH Final Exam ANSWER KEY September 2018Document25 pagesTOPNOTCH Final Exam ANSWER KEY September 2018CDNo ratings yet
- University of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - ConsortiumDocument17 pagesUniversity of Perpetual Help Rizal Jonelta Foundation School of Medicine Department of Surgery - Consortiummefav7778520No ratings yet
- 1 LiverDocument10 pages1 LiverAlbino Fulgencio Santos III100% (1)
- 2 Initial Steps PDFDocument22 pages2 Initial Steps PDFBeatrice Joy TombocNo ratings yet
- PGI Graduation 2019 FinalDocument153 pagesPGI Graduation 2019 FinalBen Paolo Cecilia RabaraNo ratings yet
- OCHA PH - Measles OutbreakDocument1 pageOCHA PH - Measles OutbreakPhilippe Ceasar C. BascoNo ratings yet
- Protein Energy MalnutritionDocument16 pagesProtein Energy MalnutritionAisha Abdullah ManzurNo ratings yet
- MicrobiologyDocument169 pagesMicrobiologyAnnaNo ratings yet
- 1ST MIDTERM BIOCHEM EVALUATION EXAMDocument2 pages1ST MIDTERM BIOCHEM EVALUATION EXAMMaryNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Case On Upper GI Bleeding: Interns Chua, EsquidaDocument59 pagesCase On Upper GI Bleeding: Interns Chua, EsquidaJoyce ChuaNo ratings yet
- Hepatobilier Ultrasound: DR - Yanto Budiman, SP - Rad, M.Kes Bagian Radiologi FKUAJ / RSAJDocument65 pagesHepatobilier Ultrasound: DR - Yanto Budiman, SP - Rad, M.Kes Bagian Radiologi FKUAJ / RSAJResNo ratings yet
- Treatment of Portal HypertensionDocument10 pagesTreatment of Portal HypertensionLourianne NcNo ratings yet
- Baveno Vii PDFDocument16 pagesBaveno Vii PDFAna ClaudiaNo ratings yet
- Portal HypertensionDocument5 pagesPortal HypertensionWendy EscalanteNo ratings yet
- Khanna 2018Document20 pagesKhanna 2018wahid akbarNo ratings yet
- Chapter 7Document34 pagesChapter 7Hima AlqahtaniNo ratings yet
- Edited HP I Fri ConfDocument85 pagesEdited HP I Fri ConfTara Oliveros Dela CruzNo ratings yet
- Portal Hypertensive Gastropathy With A Focus On Management: ReviewDocument10 pagesPortal Hypertensive Gastropathy With A Focus On Management: ReviewDevy Widiya GrafitasariNo ratings yet
- Hepatic EncephalopathyDocument5 pagesHepatic Encephalopathyliveconnectionz282No ratings yet
- Liver CirrohosisDocument157 pagesLiver CirrohosisSeema SachdevaNo ratings yet
- Understanding Liver CirrhosisDocument54 pagesUnderstanding Liver CirrhosisaprillyaNo ratings yet
- Theme 11. Portal HypertentionDocument33 pagesTheme 11. Portal HypertentionHashmithaNo ratings yet
- Varices Esophagus PDFDocument7 pagesVarices Esophagus PDFDimas ErlanggaNo ratings yet
- Portal HypertensionDocument60 pagesPortal HypertensionParul VarshneyNo ratings yet
- CT Features of Extrahepatic Arterioportal Fistula in Two CatsDocument4 pagesCT Features of Extrahepatic Arterioportal Fistula in Two CatsVennaOktaviaAnggrainiNo ratings yet
- Portal HypertensionDocument103 pagesPortal Hypertensionsolysan50% (2)
- Surgery LMRP 2019Document65 pagesSurgery LMRP 2019skNo ratings yet
- Gastrointestinal System DisordersDocument112 pagesGastrointestinal System DisordersTaate MohammedNo ratings yet
- Liver Curs 2009Document215 pagesLiver Curs 2009Mohammad_Islam87No ratings yet
- Abdominal US in Hepatobiliary DiseasesDocument76 pagesAbdominal US in Hepatobiliary DiseasesSyafari D. MangopoNo ratings yet
- Portal Hypertension SurgeryDocument6 pagesPortal Hypertension SurgeryjackSNMMCNo ratings yet
- Portal Hypotension: Clinical AssignmentDocument8 pagesPortal Hypotension: Clinical AssignmentM shayan JavedNo ratings yet
- Acute Liver Failure-1Document40 pagesAcute Liver Failure-1elizabethNo ratings yet
- CCRN-PCCN Review GastrointestinalDocument23 pagesCCRN-PCCN Review GastrointestinalGiovanni MictilNo ratings yet
- Portal Hypertension Pathogenesis and Diagnosis PDFDocument15 pagesPortal Hypertension Pathogenesis and Diagnosis PDFLizeth GirónNo ratings yet
- Diagnostic Imaging of Dogs With Suspected Por To Systemic ShuntingDocument10 pagesDiagnostic Imaging of Dogs With Suspected Por To Systemic ShuntingHospital Veterinário e Pet Shop Dr. HatoNo ratings yet
- LECTURES Liver PathophysiologyDocument118 pagesLECTURES Liver PathophysiologyTarik100% (1)
- Liver DiseaseDocument19 pagesLiver Diseasenishi kNo ratings yet