You might also like
- OR InstrumentsDocument56 pagesOR Instrumentssellyna SaidinNo ratings yet
- Newborn Care Free Online EditionDocument452 pagesNewborn Care Free Online EditionMayeso E. ChikwalikwaliNo ratings yet
- Perioperative Nursing: Rachelle M. Ganuelas RN, MANDocument66 pagesPerioperative Nursing: Rachelle M. Ganuelas RN, MANdianahazel_03No ratings yet
- Sepsis Content Concepts MapDocument3 pagesSepsis Content Concepts Mapghodghod1230% (1)
- Cardiac ArrestDocument10 pagesCardiac ArrestFebby Aulia AriefNo ratings yet
- CanulationDocument21 pagesCanulationJason Liando100% (1)
- Non-Pharmacological Pain Management PDFDocument15 pagesNon-Pharmacological Pain Management PDFEndy JuliantoNo ratings yet
- AbbreviationsDocument3 pagesAbbreviationsJade Hemmings100% (1)
- Modern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.From EverandModern Anaesthesia:: A Concise Guide to the Study and Practice of Anaesthesia.No ratings yet
- 2714 - Peripheral Venous Catheter Care Policy For AdultsDocument10 pages2714 - Peripheral Venous Catheter Care Policy For AdultssofiinhaptNo ratings yet
- IV TherapyDocument39 pagesIV TherapyChannelGNo ratings yet
- CentralVenousCatheter CVCDocument41 pagesCentralVenousCatheter CVCPraveen RavishankaranNo ratings yet
- Tracheostomy SuctioningDocument59 pagesTracheostomy SuctioningMaan LapitanNo ratings yet
- Airway ManagementDocument16 pagesAirway ManagementSuganthi ParthibanNo ratings yet
- Watchtower: The "Jensen Letters": Analysis and Commentary by Doug MasonDocument20 pagesWatchtower: The "Jensen Letters": Analysis and Commentary by Doug MasonsirjsslutNo ratings yet
- Central Line Associated Bloodstream Infections (CLABSI)Document41 pagesCentral Line Associated Bloodstream Infections (CLABSI)roslah sopiah100% (1)
- BSN3-1 Perioperative-Nursing 2021Document236 pagesBSN3-1 Perioperative-Nursing 2021Ms MedSurg Nursin100% (2)
- Vitamin KDocument1 pageVitamin Kambet100% (2)
- Accomplishment Report 2017 - IcuDocument5 pagesAccomplishment Report 2017 - IcuMikhaelEarlSantosTacordaNo ratings yet
- Drugs and Ivf Calculation: Jessica M. Dela Cruz, RN, MSNDocument10 pagesDrugs and Ivf Calculation: Jessica M. Dela Cruz, RN, MSNamal abdulrahmanNo ratings yet
- Peripheral Venous AccessDocument23 pagesPeripheral Venous AccessIan RochaNo ratings yet
- Basics of ICU CareDocument19 pagesBasics of ICU CareUmar Farooq GondalNo ratings yet
- Guidline of Management of Porta CathDocument8 pagesGuidline of Management of Porta CathroncekeyNo ratings yet
- 0347burst AbdomenDocument24 pages0347burst AbdomenSathishKumar100% (1)
- Shirish M Kawthalkar - Essentials of Clinical Pathology-Jp Medical LTD (2018)Document446 pagesShirish M Kawthalkar - Essentials of Clinical Pathology-Jp Medical LTD (2018)poopziNo ratings yet
- Central Venous CatheterizationDocument34 pagesCentral Venous CatheterizationMujeeb NangrajNo ratings yet
- Perioperative CareDocument39 pagesPerioperative CareSolomon100% (1)
- Lumbar PunctureDocument37 pagesLumbar PunctureRahul Varshney100% (1)
- Critically Ill PatientDocument31 pagesCritically Ill PatientSameh Aziz100% (2)
- Recovery Room NurseDocument5 pagesRecovery Room NurseChristin 'Kirei' AndoloNo ratings yet
- Procedure-Central Venous Access Catheter InsertionDocument18 pagesProcedure-Central Venous Access Catheter Insertionmohamad dildarNo ratings yet
- The Operating TheatreDocument30 pagesThe Operating TheatrePrincewill SeiyefaNo ratings yet
- Bladder CatheterizationDocument1 pageBladder Catheterizationlizzy596No ratings yet
- CVAD For NursesDocument54 pagesCVAD For NursesRitaLakhaniNo ratings yet
- Pharmacology For Pharmacy Technicians 2nd Edition Moscou Test BankDocument25 pagesPharmacology For Pharmacy Technicians 2nd Edition Moscou Test BankCharlesBlackbswk100% (53)
- Cholangiocarcinoma: The Right Clinical Information, Right Where It's NeededDocument40 pagesCholangiocarcinoma: The Right Clinical Information, Right Where It's NeededHan KethyanethNo ratings yet
- Peripheral Intravenous Cannulation PolicyDocument14 pagesPeripheral Intravenous Cannulation PolicyRoksana AkhterNo ratings yet
- NSO Policy FInal DraftDocument100 pagesNSO Policy FInal DraftRED STATIONNo ratings yet
- Reading Jahshan Oet CollectionDocument398 pagesReading Jahshan Oet CollectionMaria del CarmenNo ratings yet
- Fundam Nursing Skill Lab ManualDocument97 pagesFundam Nursing Skill Lab ManualBirhanu AyenewNo ratings yet
- Peripheral CannulationDocument3 pagesPeripheral Cannulationaftab siddiqueNo ratings yet
- Intravenous Cannulation: PES Institute of Medical Sciences & ResearchDocument32 pagesIntravenous Cannulation: PES Institute of Medical Sciences & Researchpavithra sureshNo ratings yet
- Antimicrobialstewardship Approachesinthe Intensivecareunit: Sarah B. Doernberg,, Henry F. ChambersDocument22 pagesAntimicrobialstewardship Approachesinthe Intensivecareunit: Sarah B. Doernberg,, Henry F. ChambersecaicedoNo ratings yet
- Caring For Your Central LineDocument20 pagesCaring For Your Central Lineapi-311857882No ratings yet
- Ivt Procedure With RationaleDocument10 pagesIvt Procedure With RationalelilileeNo ratings yet
- Surgical ScrubbingDocument2 pagesSurgical ScrubbingAnn Mayie100% (1)
- Et IntubationDocument33 pagesEt Intubationsoniya josephNo ratings yet
- EndosDocument8 pagesEndosAli ZainNo ratings yet
- Electroencephalography: Preparation of Patients and Assisting With EEGDocument15 pagesElectroencephalography: Preparation of Patients and Assisting With EEGPaul MNo ratings yet
- Anesthesia Adjuvant DrugsDocument9 pagesAnesthesia Adjuvant DrugsArdra SabuNo ratings yet
- Central LinesDocument19 pagesCentral LinesJosef TrapaniNo ratings yet
- Post Op CareDocument7 pagesPost Op CareJeraldien Diente TagamolilaNo ratings yet
- Pulmonary EmbolismDocument19 pagesPulmonary EmbolismIbrahimNo ratings yet
- Nursing Management of Skin and Parasitic DiseasesDocument14 pagesNursing Management of Skin and Parasitic Diseasesyer tagalajNo ratings yet
- Clinical Aspects of NeoplasiaDocument23 pagesClinical Aspects of NeoplasiaJahanzaib BashirNo ratings yet
- Or NursingDocument48 pagesOr NursingJenn Botal Baguidudol100% (1)
- Procedure Checklist Chapter 23: Administering Intradermal InjectionsDocument2 pagesProcedure Checklist Chapter 23: Administering Intradermal InjectionsjthsNo ratings yet
- What Is AnaesthesiaDocument27 pagesWhat Is AnaesthesiaHIRANGERNo ratings yet
- Surgical Asepsis and The Principles of Sterile TechniqueDocument25 pagesSurgical Asepsis and The Principles of Sterile TechniqueArrianne Faye RamajoNo ratings yet
- Postoperative Cognitive Dysfunction Preoperative Risk Assessment and Perioperative Risk Minimization A Pragmatic Review of The LitDocument5 pagesPostoperative Cognitive Dysfunction Preoperative Risk Assessment and Perioperative Risk Minimization A Pragmatic Review of The Litade_liaNo ratings yet
- Operating Room Personnels and Their Functions: Classification of OR TeamDocument3 pagesOperating Room Personnels and Their Functions: Classification of OR TeamRona PieNo ratings yet
- Teaching Plan On Skin GraftingDocument4 pagesTeaching Plan On Skin GraftingMaria Zamantha Gatchalian100% (1)
- Quality Improvement Project ReidDocument11 pagesQuality Improvement Project Reidapi-432051161No ratings yet
- Hemodialysis English Lesson: Assignment From The Teacher Mr. Christovel Kahuweka S.PDDocument51 pagesHemodialysis English Lesson: Assignment From The Teacher Mr. Christovel Kahuweka S.PDJovelia KojongianNo ratings yet
- B U F N & H S N: Advanced Medical Surgical NURS 337 " Emergency Department Report "Document16 pagesB U F N & H S N: Advanced Medical Surgical NURS 337 " Emergency Department Report "Yousef JafarNo ratings yet
- Deviated Nasal Septum 2Document62 pagesDeviated Nasal Septum 2Mukundan Subramanian100% (1)
- Cerebral AneurysmDocument26 pagesCerebral AneurysmJo-Anne EsguerraNo ratings yet
- Nursing Management of SeizuresDocument7 pagesNursing Management of SeizuresEcaroh Hew SmailliwNo ratings yet
- CVP MonitoringDocument4 pagesCVP Monitoringسانو روديلNo ratings yet
- Antihemophilic Factor (Human) : Ko atew-DVIDocument4 pagesAntihemophilic Factor (Human) : Ko atew-DVIFlorence LiemNo ratings yet
- Dr. Jerry PDFDocument18 pagesDr. Jerry PDFFlorence LiemNo ratings yet
- ESPEN Guidelines On Enteral Nutrition - Liver Disease PDFDocument10 pagesESPEN Guidelines On Enteral Nutrition - Liver Disease PDFFlorence LiemNo ratings yet
- Graves' Disease Graves 'PenyakitDocument43 pagesGraves' Disease Graves 'PenyakitFlorence LiemNo ratings yet
- Gejala LeukokoriaDocument37 pagesGejala LeukokoriaAnonymous mFKwUNNo ratings yet
- Administering Medications and IV FluidsDocument41 pagesAdministering Medications and IV FluidsJada RichardsNo ratings yet
- Forum: Ethamsylate and Blood Loss in Total Hip ReplacementDocument5 pagesForum: Ethamsylate and Blood Loss in Total Hip ReplacementDian NovitasariNo ratings yet
- 2010 Review ReadinessDocument75 pages2010 Review ReadinessGenesis Niogan100% (2)
- TMF HospitalDocument1 pageTMF Hospitalsurya syndicateNo ratings yet
- Product Nasivion SprayDocument5 pagesProduct Nasivion SprayMueen mohsinNo ratings yet
- Infliximab ProtDocument5 pagesInfliximab ProtQusay AbdohNo ratings yet
- Skin Erosion A Rare Long Term Complication of The Chemotherapy Port 305Document1 pageSkin Erosion A Rare Long Term Complication of The Chemotherapy Port 305Medtext PublicationsNo ratings yet
- New Pediatric Guideline Hargeisa Group Hospital by DR NelsonDocument54 pagesNew Pediatric Guideline Hargeisa Group Hospital by DR NelsonKhadar mohamedNo ratings yet
- Alaris Medley Prog Module 8000 Version 4aDocument51 pagesAlaris Medley Prog Module 8000 Version 4aAlondra MagañaNo ratings yet
- European Resuscitation Council Guidelines 2021 PaDocument61 pagesEuropean Resuscitation Council Guidelines 2021 Paresti illahiNo ratings yet
- The Golden Hours in Treatment Am J Gastroenterol 2012 Aug 107 (8) 1146Document5 pagesThe Golden Hours in Treatment Am J Gastroenterol 2012 Aug 107 (8) 1146hojadecoca1313No ratings yet
- 2022 ISPAD Clinical Practice Consensus Guidelines 2022Document70 pages2022 ISPAD Clinical Practice Consensus Guidelines 2022WenSarmientoBNo ratings yet
- Medication Incompatibility in Intravenous Lines in A Paediatric Intensive Care Unit (PICU) of Indonesian Hospital (Kel.8)Document11 pagesMedication Incompatibility in Intravenous Lines in A Paediatric Intensive Care Unit (PICU) of Indonesian Hospital (Kel.8)Rotama GurningNo ratings yet
- Diseases of The Newborn Part2Document6 pagesDiseases of The Newborn Part2sarguss14100% (1)
- TCI DiprivanDocument74 pagesTCI DiprivanVan Basten ArdiansyachNo ratings yet
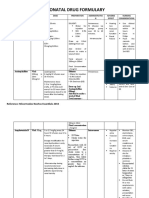
- Neonatal Drug FormularyDocument6 pagesNeonatal Drug FormularyLucian CaelumNo ratings yet
- Bamlanivimab EUA Healthcare Provider Fact Sheet - 0Document23 pagesBamlanivimab EUA Healthcare Provider Fact Sheet - 0Farman JaaferNo ratings yet
- NP 3Document20 pagesNP 3MENARDNo ratings yet
- OPERATING ROOM TECHNIQUES NCM 112aDocument37 pagesOPERATING ROOM TECHNIQUES NCM 112aGrape JuiceNo ratings yet
- Principles of Medication AdministrationDocument10 pagesPrinciples of Medication AdministrationEarl BenedictNo ratings yet