You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Approach To The Patient With DyspneaDocument22 pagesApproach To The Patient With DyspneaLuis Gerardo Alcalá GonzálezNo ratings yet
- Nursing Process Record - Nursing FundamentalsDocument17 pagesNursing Process Record - Nursing FundamentalsheidiheffNo ratings yet
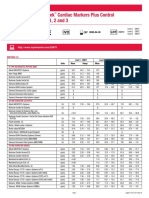
- Liquichek Cardiac Markers Plus Control Levels 1, 2 and 3: MethodDocument4 pagesLiquichek Cardiac Markers Plus Control Levels 1, 2 and 3: MethodSaifoel RahmanNo ratings yet
- Vasoactive PeptidesDocument65 pagesVasoactive PeptidesJayrine MonteroNo ratings yet
- Normal Reference Ranges For Laboratory Values in PregnancyDocument5 pagesNormal Reference Ranges For Laboratory Values in PregnancyPedro Canudo SenaNo ratings yet
- Noncardiogenic Pulmonary Edema - UpToDateDocument17 pagesNoncardiogenic Pulmonary Edema - UpToDateStefani AtlleNo ratings yet
- Attending COPD Exacerbation ModuleDocument9 pagesAttending COPD Exacerbation ModuleJonathan AiresNo ratings yet
- Part 1 SAQs Specimen QuestionsDocument79 pagesPart 1 SAQs Specimen Questionsخولة رشيد العيسى100% (2)
- Evaluation of The Adult With Dyspnea in The Emergency DepartmentDocument16 pagesEvaluation of The Adult With Dyspnea in The Emergency DepartmentmericenteNo ratings yet
- Philip Kalra PDFDocument38 pagesPhilip Kalra PDFDennis JakeNo ratings yet
- Update On PPHN: Mechanisms and Treatment: Jayasree Nair, MBBS, MD, and Satyan Lakshminrusimha, MDDocument14 pagesUpdate On PPHN: Mechanisms and Treatment: Jayasree Nair, MBBS, MD, and Satyan Lakshminrusimha, MDhasan bukhoriNo ratings yet
- Acute Heart Failure WORKBOOKDocument28 pagesAcute Heart Failure WORKBOOKFadhlan ABNo ratings yet
- AstronautDocument11 pagesAstronautFlorescu VladimirNo ratings yet
- Heart Failure: Definition and EpidemiologyDocument6 pagesHeart Failure: Definition and EpidemiologyIshwarya SivakumarNo ratings yet
- Missing ValuesDocument16 pagesMissing ValuesPanagiotis KarathymiosNo ratings yet
- Copd and Cor PulmonalDocument14 pagesCopd and Cor PulmonalAldi RafaelNo ratings yet
- Assessment of Breathlessness Clinical Pathway Assessment HandoutDocument8 pagesAssessment of Breathlessness Clinical Pathway Assessment HandoutShivaniNo ratings yet
- Diastolic Dysfunction Heart FailureDocument46 pagesDiastolic Dysfunction Heart FailureChadi Alraies100% (4)
- Acute Pulmonary OdemaDocument9 pagesAcute Pulmonary OdemaAnonymous ysrxggk21cNo ratings yet
- International Journal of Cardiology: ArticleinfoDocument5 pagesInternational Journal of Cardiology: ArticleinfoWiyosa RusdiNo ratings yet
- Gnaps EmedicineDocument13 pagesGnaps Emedicineharyanti lupitaNo ratings yet
- Noninvasive Mechanical Ventilation and Difficult Weaning in Critical CareDocument442 pagesNoninvasive Mechanical Ventilation and Difficult Weaning in Critical CareCritical Group100% (8)
- 10-Primary Care - AAFP Flashcards - Quizlet PDFDocument870 pages10-Primary Care - AAFP Flashcards - Quizlet PDFehabb350% (2)
- Renal Siadh Di CSWDocument54 pagesRenal Siadh Di CSWRizka Nurul Firdaus100% (1)
- NCLEX Compiled QuestionsDocument67 pagesNCLEX Compiled Questionsjulie cruzNo ratings yet
- Q SofaDocument9 pagesQ SofadarlingcarvajalduqueNo ratings yet
- Acute Care TestingDocument222 pagesAcute Care TestingAdel ChaabaneNo ratings yet
- BNP in CKDDocument6 pagesBNP in CKDDedy ShauqiNo ratings yet
- Biomarker Discovery in Cardio-Oncology.Document8 pagesBiomarker Discovery in Cardio-Oncology.Ștefan SpînuNo ratings yet
- A Guide To Peripheral EdemaDocument7 pagesA Guide To Peripheral Edemadanny17phNo ratings yet