You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Choosing Blood Pressure MedicationsDocument8 pagesChoosing Blood Pressure MedicationsbhaskarNo ratings yet
- Top 200 DrugsDocument12 pagesTop 200 DrugsYudah Israel100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Empr Prescriber's EditionDocument420 pagesEmpr Prescriber's EditionPatel Pratyk100% (1)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Meniere's Disease - PowerpointDocument13 pagesMeniere's Disease - PowerpointDe Sesto Rhys CarloNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Pearls For NCLEX Review in Publisher March PDFDocument34 pagesThe Pearls For NCLEX Review in Publisher March PDFKim Medairos100% (3)
- Contest Prep Show Day Holding The PeakDocument24 pagesContest Prep Show Day Holding The Peakthekid skyNo ratings yet
- Nutrient Depletion GuideDocument2 pagesNutrient Depletion GuideMichael CabarlesNo ratings yet
- Meniere's Case Study Written ReportDocument16 pagesMeniere's Case Study Written ReportJoie JoieNo ratings yet
- Family MedicineDocument156 pagesFamily MedicinedtriggNo ratings yet
- Katrina D. Varon Bs-Nursing 2Document13 pagesKatrina D. Varon Bs-Nursing 2Marc FresNo ratings yet
- Top 200 Drugs in OrderDocument7 pagesTop 200 Drugs in OrderEamon BarkhordarianNo ratings yet
- Table Heart MedsDocument5 pagesTable Heart MedsHazel Ann MolinoNo ratings yet
- 2 DRUGS For HYPERTENSIONDocument4 pages2 DRUGS For HYPERTENSIONMushy_ayaNo ratings yet
- Medication Induced Nutrient DepletionDocument3 pagesMedication Induced Nutrient Depletionr.sorghabiNo ratings yet
- TriamtereneDocument2 pagesTriamtereneapi-3797941No ratings yet
- Cozaar 25 MG: What Is Losartan (Cozaar) ?Document25 pagesCozaar 25 MG: What Is Losartan (Cozaar) ?nyzgirl17No ratings yet
- Dyrenium Triamterene Drug CardDocument1 pageDyrenium Triamterene Drug CardSheri490No ratings yet
- Tufts by Therapeutic ClassDocument56 pagesTufts by Therapeutic ClassJames LindonNo ratings yet
- Adverse Reactions To DiureticsDocument8 pagesAdverse Reactions To DiureticsDimas RizkyNo ratings yet
- Physics and ChemistryDocument4 pagesPhysics and ChemistryshahabNo ratings yet
- Farmakoterapi Sistem RenalDocument89 pagesFarmakoterapi Sistem RenalNhovieNhowaaNo ratings yet
- Daftar Obat Anti Hipertensi PDFDocument7 pagesDaftar Obat Anti Hipertensi PDFPietra Jaya100% (1)
- B.Veletsis-Anthem MediBlue RX Plus (PDP) PDFDocument9 pagesB.Veletsis-Anthem MediBlue RX Plus (PDP) PDFdonnaNo ratings yet
- B.Veletsis-Humana Walmart Value RX Plan (PDP) PDFDocument8 pagesB.Veletsis-Humana Walmart Value RX Plan (PDP) PDFdonnaNo ratings yet
- Antihypertensives: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimDocument31 pagesAntihypertensives: 2005 Wiley-Vch Verlag GMBH & Co. Kgaa, WeinheimjaimeNo ratings yet
- Tugas Penilaian Status GiziDocument12 pagesTugas Penilaian Status GiziZahra ZahiraNo ratings yet
- Top 200 DrugsDocument14 pagesTop 200 DrugsDavid NguyenNo ratings yet
- AntihypertensivesDocument35 pagesAntihypertensivesjanuajipatriaNo ratings yet
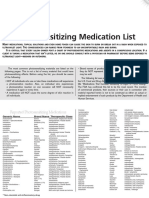
- Photosensitizing Medication ListDocument3 pagesPhotosensitizing Medication ListDimas RfNo ratings yet
- Light Sensitive Drug-02Document6 pagesLight Sensitive Drug-02abutalibNo ratings yet