You might also like
- Spinal Tuberculosis (Pott's Disease)Document19 pagesSpinal Tuberculosis (Pott's Disease)Komalah ChenasammyNo ratings yet
- MateriDocument39 pagesMateriDR BASUKINo ratings yet
- Stemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVDocument35 pagesStemi Acute Coronary Syndrome: Dr. Muh A Sungkar, SPPD, SPJP, KKVCoass BonamNo ratings yet
- Gasem MH HANTA Salatiga 2019Document43 pagesGasem MH HANTA Salatiga 2019ChristianNo ratings yet
- SS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFDocument34 pagesSS II.1.1 Update On Typhoid Management - Dr. Adityo Susilo, SpPD-KPTI PDFWisnu Yudho HNo ratings yet
- Essensial Hypertension Pathogenesis and PathophsiologyDocument22 pagesEssensial Hypertension Pathogenesis and PathophsiologyAmeliana KamaludinNo ratings yet
- HFpEF MeDocument28 pagesHFpEF MeRidwan YasinNo ratings yet
- ADPKDDocument75 pagesADPKDVenkataramanan KrishnamoorthyNo ratings yet
- Immunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIDocument29 pagesImmunopatologi Sepsis - DR Nur Farhanah SPPD K-PTIanita tri hastutiNo ratings yet
- Rheumatoid Arthritis: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 2/ 11/ 2020Document54 pagesRheumatoid Arthritis: Hozan Jaza MSC Clinical Pharmacy College of Pharmacy 2/ 11/ 2020Alan K Mhamad100% (1)
- MyocarditisDocument1 pageMyocarditisintrovoyz041No ratings yet
- Clinical Aspects of PneumothoraxDocument3 pagesClinical Aspects of PneumothoraxelisabethNo ratings yet
- Diabetic NephropathyDocument5 pagesDiabetic NephropathydnllkzaNo ratings yet
- Everything You Need to Know About DyspneaDocument34 pagesEverything You Need to Know About DyspneaAlvin BrilianNo ratings yet
- Case AnalysisDocument12 pagesCase AnalysisFroilan TaracatacNo ratings yet
- Ventikular Septal Defect FixDocument18 pagesVentikular Septal Defect FixPutri Sari DewiNo ratings yet
- LA Myxoma Case PresentationDocument34 pagesLA Myxoma Case PresentationWiwik Puji LestariNo ratings yet
- Pathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsDocument2 pagesPathophysiology Diagram of Kawasaki Disease: Precipitating Factors: Predisposing FactorsAb Staholic Boii100% (1)
- UrethritisDocument11 pagesUrethritisgreggy_rebel17No ratings yet
- Wound Dressing JurnalDocument32 pagesWound Dressing JurnalMuhsinAnisNo ratings yet
- Hypertension and Cardiovascular DiseaseDocument99 pagesHypertension and Cardiovascular DiseaseMiguel CuevasNo ratings yet
- Perforated Peptic Ulcer Symptoms and DiagnosisDocument68 pagesPerforated Peptic Ulcer Symptoms and DiagnosisSaibo BoldsaikhanNo ratings yet
- Penetrating Chest Trauma With Massive Hemothorax by A Small StoneDocument2 pagesPenetrating Chest Trauma With Massive Hemothorax by A Small Stoneputri firda erlinaNo ratings yet
- Dr. Sunatrio - Management Hypovolemic ShockDocument59 pagesDr. Sunatrio - Management Hypovolemic ShockArga Putra SaboeNo ratings yet
- Spinal Cord Injury Rehab GoalsDocument17 pagesSpinal Cord Injury Rehab GoalsRaghu Nadh100% (1)
- PneumoniaDocument1 pagePneumoniamai_senoNo ratings yet
- Normal Values of CBCDocument1 pageNormal Values of CBCCherr NollNo ratings yet
- Asthma Case ReportDocument21 pagesAsthma Case ReportbungaamiliasuariNo ratings yet
- Acute and Chronic Pancreatitis ShirleyDocument6 pagesAcute and Chronic Pancreatitis ShirleyVictor AladejanaNo ratings yet
- Cardiovascular Disease in The ElderlyDocument18 pagesCardiovascular Disease in The ElderlynfacmaNo ratings yet
- Pulmonary Hypertension: Causes, Symptoms, Diagnosis & TreatmentDocument3 pagesPulmonary Hypertension: Causes, Symptoms, Diagnosis & TreatmentJiezl Abellano AfinidadNo ratings yet
- Hiatal Hernia AchalasiaDocument22 pagesHiatal Hernia AchalasiaDhen MarcNo ratings yet
- Histoplasmosis Characteristics Pathogenesis Treatment ChallengesDocument19 pagesHistoplasmosis Characteristics Pathogenesis Treatment ChallengesKathzkaMaeAgcaoiliNo ratings yet
- Coughs and Colds Nurse Management of Upper Respiratory Tract InfectionDocument3 pagesCoughs and Colds Nurse Management of Upper Respiratory Tract InfectionMichael Anthony ErmitaNo ratings yet
- CellulitisDocument5 pagesCellulitisaimigdragonNo ratings yet
- Diabetes PathoDocument2 pagesDiabetes Pathodrewcel100% (1)
- Deep Venous Thrombosis Harrison'sDocument3 pagesDeep Venous Thrombosis Harrison'sMaria Agustina Sulistyo WulandariNo ratings yet
- Emerging, Re-emerging Diseases and NTDs in IndonesiaDocument32 pagesEmerging, Re-emerging Diseases and NTDs in IndonesiaMelia100% (1)
- Pneumocytis Carinii PneumoniaDocument26 pagesPneumocytis Carinii Pneumoniafrancis00090No ratings yet
- Causes, Symptoms & Types of Cerebral InfarctionDocument2 pagesCauses, Symptoms & Types of Cerebral InfarctionMarie Aurora Gielbert MarianoNo ratings yet
- Predisposing Conditions, Management and Prevention of Chronic Kidney DiseaseDocument52 pagesPredisposing Conditions, Management and Prevention of Chronic Kidney DiseaseSaad MotawéaNo ratings yet
- Abdominal Compartment SyndromeDocument7 pagesAbdominal Compartment Syndromemezgebu alemnehNo ratings yet
- STEMI anteroseptalDocument42 pagesSTEMI anteroseptalWarren LieNo ratings yet
- CVD Bleed Case StudyDocument25 pagesCVD Bleed Case StudyMargaret Jenaw JenawNo ratings yet
- Case Study 4th Year 1st Sem 2 Final FixDocument30 pagesCase Study 4th Year 1st Sem 2 Final FixHerschel QuerimitNo ratings yet
- Clinical Approach to HypertensionDocument16 pagesClinical Approach to HypertensionShradha KhuranaNo ratings yet
- Pityriasis Versicolor Part 1Document9 pagesPityriasis Versicolor Part 1Sopna Zenith0% (1)
- Roseola PDFDocument1 pageRoseola PDFLili PredescuNo ratings yet
- BFCDocument8 pagesBFCIrene GunongNo ratings yet
- Disseminated Intravascular CoagulationDocument8 pagesDisseminated Intravascular CoagulationMade NoprianthaNo ratings yet
- Referat: Pneumonia in ElderlyDocument41 pagesReferat: Pneumonia in Elderlyathieqah say-syahidahNo ratings yet
- Leprosy CHNDocument14 pagesLeprosy CHNPhillip ChingNo ratings yet
- Tension Pneumothorax PDFDocument2 pagesTension Pneumothorax PDFClarissa Aileen Caliva AdoraNo ratings yet
- Kuliah Thrombosis 2015 NNDocument39 pagesKuliah Thrombosis 2015 NNBeladiena Citra SiregarNo ratings yet
- Effects of Aging On The Cardiovascular SystemDocument40 pagesEffects of Aging On The Cardiovascular SystemRendy Grinaldi FadilahNo ratings yet
- Pathophysiology of HFDocument40 pagesPathophysiology of HFHayaNo ratings yet
- Cardiovascular - Anatomy & PhysiologyDocument23 pagesCardiovascular - Anatomy & PhysiologySanthoshi Sadhanaa Sankar100% (1)
- NSG 210 Study GuideDocument25 pagesNSG 210 Study GuideyasserNo ratings yet
- Patofisiologi Sistem KardiovaskularDocument157 pagesPatofisiologi Sistem KardiovaskularNyanmaruNo ratings yet
- CVS DOs RevisedDocument88 pagesCVS DOs RevisedTaate MohammedNo ratings yet
- 2007 Obat Pada ManulaDocument62 pages2007 Obat Pada ManulaVania OktavianiNo ratings yet
- 2007 Obat Pada ManulaDocument62 pages2007 Obat Pada ManulaVania OktavianiNo ratings yet
- Station2 Herpes ZoosterDocument4 pagesStation2 Herpes ZoosterVania OktavianiNo ratings yet
- Jurnal ReadingDocument18 pagesJurnal ReadingVania OktavianiNo ratings yet
- Jama Statin and Stroke Prevention SupplementDocument17 pagesJama Statin and Stroke Prevention SupplementMesan KoNo ratings yet
- Cardio Post TestDocument13 pagesCardio Post TestCharme Jean RaygonNo ratings yet
- AHA ACLS Precourse Self Assessment Answers 2023Document32 pagesAHA ACLS Precourse Self Assessment Answers 2023R100% (4)
- Ecg MCQSDocument2 pagesEcg MCQSZafar Iqbal Manj100% (2)
- Heart Failure in ChildrenDocument27 pagesHeart Failure in ChildrendenakarinaNo ratings yet
- Congenital Heart DiseaseDocument5 pagesCongenital Heart Diseasesarguss14100% (1)
- Deadly PE Blood Clot Blocks Lung ArteriesDocument1 pageDeadly PE Blood Clot Blocks Lung ArteriesTrisha VergaraNo ratings yet
- Learning Cardiac Auscultation by Taylor and Springer From Am MedicalbooksDocument327 pagesLearning Cardiac Auscultation by Taylor and Springer From Am MedicalbooksSivakumar Gounden100% (1)
- Nennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyDocument10 pagesNennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyBayu IsmoyoNo ratings yet
- Daftar Pustaka LailyDocument4 pagesDaftar Pustaka LailyOsbon SitumorangNo ratings yet
- CardiovascularDocument155 pagesCardiovascularEric VeranoNo ratings yet
- Arrhythmia and Conduction Disturbance-AAL-UPH2020Document100 pagesArrhythmia and Conduction Disturbance-AAL-UPH2020Ammar GalihNo ratings yet
- Surgery in Elderly 2Document41 pagesSurgery in Elderly 2Zeba NaveedNo ratings yet
- Assessment of Heart & Neck VesselsDocument4 pagesAssessment of Heart & Neck VesselsCardio GodNo ratings yet
- GREY BOOK August 2017 66thDocument146 pagesGREY BOOK August 2017 66thxedoyis969No ratings yet
- Carotid Sinus Massage Leaflet PDFDocument3 pagesCarotid Sinus Massage Leaflet PDFkunkkonkNo ratings yet
- Quiz 2Document5 pagesQuiz 2Ani MepharishviliNo ratings yet
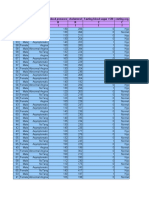
- Age Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I IDocument14 pagesAge Sex Chest Pain Type Blood Pressure Cholesterol Fasting Blood Sugar 120 Resting Ecg R C C R R C C I I I I I I Isantu4_1111No ratings yet
- Pathophysiology of Hypertensive Cardiovascular Disease PDFDocument3 pagesPathophysiology of Hypertensive Cardiovascular Disease PDFAbdelrahman GalalNo ratings yet
- Basic EKG Review: Identify Rhythms & InterventionsDocument31 pagesBasic EKG Review: Identify Rhythms & Interventionsmeb100% (1)
- Clinical Exam NotesDocument222 pagesClinical Exam Notesakansha_bhargava_6100% (1)
- Hemodynamic Unstable Patient Following ArrhythmiaDocument30 pagesHemodynamic Unstable Patient Following Arrhythmialew chin hongNo ratings yet
- STROKEDocument9 pagesSTROKEhillary elsaNo ratings yet
- Lampung University Medical Faculty Left Hemiparesis Due to Hemorrhagic StrokeDocument10 pagesLampung University Medical Faculty Left Hemiparesis Due to Hemorrhagic StrokeKrisna ajiNo ratings yet
- Electrocardiogram: Dr. PacnaDocument13 pagesElectrocardiogram: Dr. PacnaEcel AggasidNo ratings yet
- CPG Coronary Artery DiseaseDocument44 pagesCPG Coronary Artery DiseaseReuter Lloyd MarianoNo ratings yet
- VT Bradycardias AnswDocument128 pagesVT Bradycardias AnswJoshua-Majid ShahbaziNo ratings yet
- CIMT and StrokeDocument3 pagesCIMT and StrokeNurul RakhmawatiNo ratings yet
- Pathophysiology of Atrial Septal DefectDocument2 pagesPathophysiology of Atrial Septal Defectbobtaguba50% (2)
- EKG Arrhythmia Identification GuideDocument47 pagesEKG Arrhythmia Identification Guidemithaa octoviagnesNo ratings yet