You might also like
- 35 Nclex QuestionsDocument6 pages35 Nclex Questionsjohnnymyunghee0% (1)
- Community PsychiatryDocument45 pagesCommunity PsychiatrySarvess MuniandyNo ratings yet
- Final Exam Studyguide Spring 2017Document5 pagesFinal Exam Studyguide Spring 2017Nataraj LoganathanNo ratings yet
- Buffer KSP ProbDocument4 pagesBuffer KSP ProbFitria Rahma DewiNo ratings yet
- Gastrointestinal and HepatobiliaryDocument54 pagesGastrointestinal and Hepatobiliaryjeshema100% (2)
- Endotracheal TubeDocument19 pagesEndotracheal TubeSarvess Muniandy100% (1)
- Postpartum Hemorrhage PPHDocument70 pagesPostpartum Hemorrhage PPHLoungayvan BatuyogNo ratings yet
- Hyperemesis Gravidarum: Bleeding Complications of PregnancyDocument6 pagesHyperemesis Gravidarum: Bleeding Complications of PregnancykirbsNo ratings yet
- Antepartum Fetal Assessment 2018Document39 pagesAntepartum Fetal Assessment 2018amena mahmoudNo ratings yet
- Final Adult Health 1 HESI InfoDocument2 pagesFinal Adult Health 1 HESI InfoJamie Antonini GrantNo ratings yet
- Ch. 1, Lesson 1: What Is The Next Gen NCLEXDocument4 pagesCh. 1, Lesson 1: What Is The Next Gen NCLEXChantelNo ratings yet
- Endocrine System: Major Hormone Secreting Glands: 1. HypothalamusDocument5 pagesEndocrine System: Major Hormone Secreting Glands: 1. HypothalamusSTEFFI GABRIELLE GOLEZNo ratings yet
- Management of Anovulatory Infertility and Polycystic Ovary DiscsDocument41 pagesManagement of Anovulatory Infertility and Polycystic Ovary Discsapi-3705046100% (1)
- Ati QuestionsDocument2 pagesAti Questionsnjames44No ratings yet
- CH 14 Wardand HInsley Maternity Power PointDocument25 pagesCH 14 Wardand HInsley Maternity Power PointJonalyn ChewacheoNo ratings yet
- Alcohol Use DisorderDocument68 pagesAlcohol Use DisorderSarvess Muniandy100% (3)
- Monitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineDocument58 pagesMonitoring The Progress of Labor: Marissa Villacarlos Nualla, MD, Fpogs, Fpsuog Mcu-College of MedicineRozzie ReyesNo ratings yet
- Fluids and ElectrolytesDocument128 pagesFluids and Electrolytesmd6ztpydckNo ratings yet
- Fetal Monitoring Orientation Day-1Document50 pagesFetal Monitoring Orientation Day-1Scott CalfeeNo ratings yet
- UntitledDocument41 pagesUntitledvioletdeocaresNo ratings yet
- 2) QuestionsDocument95 pages2) Questionsgita safiraNo ratings yet
- Dysrhythmias: Se Admin Anticoagulante, Cardioversion As PrescribedDocument10 pagesDysrhythmias: Se Admin Anticoagulante, Cardioversion As Prescribedyaneidys perezNo ratings yet
- Isotonic, HypotDocument4 pagesIsotonic, HypotSannyjale BaldozaNo ratings yet
- ATI RN Nursing Care of Children Online Practice 2019 ADocument4 pagesATI RN Nursing Care of Children Online Practice 2019 Aianshirow834No ratings yet
- Hematologic System2Document70 pagesHematologic System2Jesus Mario LopezNo ratings yet
- Parag Dairy TrainingDocument30 pagesParag Dairy TrainingVarisha Saleem67% (9)
- PB 20Document10 pagesPB 20Cheng CapunoNo ratings yet
- Acid and Base Balance and ImbalanceDocument38 pagesAcid and Base Balance and ImbalanceMustafa KhandgawiNo ratings yet
- Acid-Base Balance + Arterial Blood GasesDocument30 pagesAcid-Base Balance + Arterial Blood GasesQusai IbraheemNo ratings yet
- VSim SARAH LIN For Nursing - Health Assessment POST QUIZDocument5 pagesVSim SARAH LIN For Nursing - Health Assessment POST QUIZWen RodsaNo ratings yet
- Fetal Heart Rate Interpretation Adaptation To LaborDocument36 pagesFetal Heart Rate Interpretation Adaptation To Laboryolondanic100% (1)
- Buffer System: Danica Alyssa C. Cruz, RMTDocument27 pagesBuffer System: Danica Alyssa C. Cruz, RMTDanica Alyssa CruzNo ratings yet
- Physiologic Transition From Intrauterine To Extrauterine LifeDocument12 pagesPhysiologic Transition From Intrauterine To Extrauterine Lifeyhojar PisfilNo ratings yet
- IV Infusion SolutionDocument8 pagesIV Infusion SolutionmohammedNo ratings yet
- Jennifer Portillo Health Assessment VocabularyDocument9 pagesJennifer Portillo Health Assessment VocabularyJennifer PortilloNo ratings yet
- Nervous SystemDocument42 pagesNervous SystemAbobakr AlobeidNo ratings yet
- Gynaecology & Obstetrics Sorted Questions 8 SemesterDocument4 pagesGynaecology & Obstetrics Sorted Questions 8 SemesterSaikat MondalNo ratings yet
- Worksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Document3 pagesWorksheet To Accompany FHR Review Video: Emerald Spangler May 6, 2021Emerald SpanglerNo ratings yet
- Diabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManDocument66 pagesDiabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManElvis J. DavisNo ratings yet
- Asthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The AsthmaDocument27 pagesAsthma That Disappears Between Ages 6-8 - Bronchioles Grew & Resolved The Asthmasimonedarling100% (1)
- MohquDocument8 pagesMohquSunil WesleyNo ratings yet
- TOLACDocument10 pagesTOLACmariaNo ratings yet
- 52 Nclex ReviewDocument1 page52 Nclex ReviewedobleNo ratings yet
- NCLEXDocument11 pagesNCLEXPrince Charles AbalosNo ratings yet
- NURS 3337 Day1 WorkbookDocument18 pagesNURS 3337 Day1 WorkbookEmerald Holly TagoNo ratings yet
- Iron Deficiency AnemiaDocument5 pagesIron Deficiency AnemiaHeather RogersNo ratings yet
- Endocrine System Study GuideDocument5 pagesEndocrine System Study GuideClaudia SanchezNo ratings yet
- Complications of LaborDocument54 pagesComplications of Laborallie-jones-6489100% (2)
- Menopause Concept MapDocument1 pageMenopause Concept MapBritanny NelsonNo ratings yet
- 3 Fluids and Electrolytes PPDocument112 pages3 Fluids and Electrolytes PPjcodoyNo ratings yet
- Physiologic Transition From Intrauterine To Extrauterine LifeDocument6 pagesPhysiologic Transition From Intrauterine To Extrauterine LifeGina M. TañedoNo ratings yet
- Post Partum Hemorrhage Med Students 85768Document37 pagesPost Partum Hemorrhage Med Students 85768salijanstarNo ratings yet
- UTI On A Background of Obstructive NephropathyDocument26 pagesUTI On A Background of Obstructive NephropathyAminath MeesanNo ratings yet
- NclexDocument4 pagesNclexihatetouNo ratings yet
- Surgery - FirecrackerDocument73 pagesSurgery - FirecrackerLucas HoldereggerNo ratings yet
- Nancy E Fay MD Facog Division of Reproductive MedicineDocument32 pagesNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoNo ratings yet
- Maternity Questions and AnswerDocument5 pagesMaternity Questions and AnswerLovaine WilliamsNo ratings yet
- Fluid, Electrolyte, and Acid Balance SherwoodDocument32 pagesFluid, Electrolyte, and Acid Balance SherwoodEvan PermanaNo ratings yet
- Global Nursing Pediatrics. Nclex - RNDocument14 pagesGlobal Nursing Pediatrics. Nclex - RNNANANo ratings yet
- Hypertension Disorders in PregnancyDocument51 pagesHypertension Disorders in Pregnancyinshu9No ratings yet
- Cesarean Section PrimaryDocument33 pagesCesarean Section PrimaryKazvin Carl PeraltaNo ratings yet
- Chapter 52 Endocrine Disorders Unit 1Document55 pagesChapter 52 Endocrine Disorders Unit 1Glory Mimi100% (1)
- Seminar, CBD, MGT & Bedside GroupDocument3 pagesSeminar, CBD, MGT & Bedside GroupSarvess MuniandyNo ratings yet
- (ORT&PSY) End-Posting Examination Questions (R2G4)Document9 pages(ORT&PSY) End-Posting Examination Questions (R2G4)Sarvess MuniandyNo ratings yet
- 1.analgesia in ObstetricDocument25 pages1.analgesia in ObstetricSarvess MuniandyNo ratings yet
- Secondary TuberculosisDocument11 pagesSecondary TuberculosisSarvess MuniandyNo ratings yet
- Enzyme AssayDocument1 pageEnzyme AssaySarvess MuniandyNo ratings yet
- Individual Assignment Cover Sheet FISDocument1 pageIndividual Assignment Cover Sheet FISSarvess MuniandyNo ratings yet
- Individual Assignment Front Page FISDocument1 pageIndividual Assignment Front Page FISSarvess MuniandyNo ratings yet
- Reasons Why You (M.Sarvesswara) Should Score 9A+ in Your Spm.....Document1 pageReasons Why You (M.Sarvesswara) Should Score 9A+ in Your Spm.....Sarvess MuniandyNo ratings yet
- ChristmasDocument3 pagesChristmasSarvess MuniandyNo ratings yet
- Monoprotic Acid-Base Equilibria: 1. Strong Acids & Bases: Dilemma in Calculating The PH of Strong Acids & BasesDocument15 pagesMonoprotic Acid-Base Equilibria: 1. Strong Acids & Bases: Dilemma in Calculating The PH of Strong Acids & BasesSkygazerNo ratings yet
- Philippine Integrated Nurse Licensure ExaminationDocument96 pagesPhilippine Integrated Nurse Licensure Examinationmhiersalyn mirulNo ratings yet
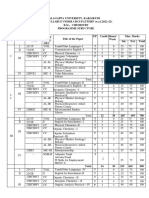
- 22 B.SC., ChemistryDocument46 pages22 B.SC., ChemistryK KANNANNo ratings yet
- ComplexoDocument14 pagesComplexoFamiFatwaNo ratings yet
- 223 FullDocument27 pages223 FullAlberto HernandezNo ratings yet
- Analytical Errors & Validation of Analytical ProceduresDocument61 pagesAnalytical Errors & Validation of Analytical ProceduresMtw WondNo ratings yet
- BPSC PharmacyDocument2 pagesBPSC PharmacyShadman RhamanNo ratings yet
- Xi 7 GTP TELDocument24 pagesXi 7 GTP TELdanielyskim1119No ratings yet
- Soil Test Interpretation EUROCODE 1999Document8 pagesSoil Test Interpretation EUROCODE 1999RanoulfoNo ratings yet
- Part - I: Subjective Questions: Section (A) : Buffer Solution & Buffer CapacityDocument12 pagesPart - I: Subjective Questions: Section (A) : Buffer Solution & Buffer Capacitypankaj agarwalNo ratings yet
- Enzymatic Activity of Salivary AmylaseDocument7 pagesEnzymatic Activity of Salivary AmylaseMaria Christina Paine80% (5)
- Hydroxyl Radical Scavenging ActivityDocument5 pagesHydroxyl Radical Scavenging ActivityManish Kumar DubeyNo ratings yet
- Phe Ethanol Fuel AN PHE ENDocument4 pagesPhe Ethanol Fuel AN PHE ENkevinNo ratings yet
- R19 Regulations Course Structure and Syllabi of B. PharmacyDocument190 pagesR19 Regulations Course Structure and Syllabi of B. PharmacySuresh VickeyNo ratings yet
- MANUAL PhmetroDocument40 pagesMANUAL PhmetroAndré AriasNo ratings yet
- Quantitative Determination of Total Hardness in Drinking Water by Complexometric EDTA TitrationDocument14 pagesQuantitative Determination of Total Hardness in Drinking Water by Complexometric EDTA Titrationabcd efgNo ratings yet
- Ionic Equilibrium: NEET 2020Document22 pagesIonic Equilibrium: NEET 2020Prabodh GuptNo ratings yet
- Astm D3242-23Document6 pagesAstm D3242-23ariniNo ratings yet
- SCHA022 Course GuidelinesDocument20 pagesSCHA022 Course Guidelinesvulkaan van huisNo ratings yet
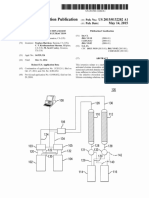
- Patent Application Publication (10) Pub. No.: US 2015/0132202 A1Document17 pagesPatent Application Publication (10) Pub. No.: US 2015/0132202 A1María Alicia Mora VergaraNo ratings yet
- Common Ion EffectDocument2 pagesCommon Ion EffectJames Eullaran100% (1)
- 1972 - Bazaral, Hamburger - Standardization and Stability of Immunoglobulin E (IgE)Document3 pages1972 - Bazaral, Hamburger - Standardization and Stability of Immunoglobulin E (IgE)pond_1993No ratings yet
- Acids, Bases and BuffersDocument20 pagesAcids, Bases and BuffersEzekoko ChineseNo ratings yet
- CAPE Chemistry Unit Two Paper OnesDocument153 pagesCAPE Chemistry Unit Two Paper OnesSam RamgatteeNo ratings yet
- Ebook Original PDF Chemical Principles 8Th Edition by Steven S Zumdahl All Chapter PDF Docx KindleDocument41 pagesEbook Original PDF Chemical Principles 8Th Edition by Steven S Zumdahl All Chapter PDF Docx Kindlericky.houck368100% (20)
- What Is A Gram Atom? Why Is The Concept of Gram Atoms Useful in Chemistry? AnswerDocument75 pagesWhat Is A Gram Atom? Why Is The Concept of Gram Atoms Useful in Chemistry? Answeryaseen shahNo ratings yet
- Development of Calibration and Standard Addition Polarographic Determination of Ascorbic AcidDocument5 pagesDevelopment of Calibration and Standard Addition Polarographic Determination of Ascorbic AcidDely GusnaNo ratings yet