You might also like
- 05 - Sle, DMZ, PHSDocument157 pages05 - Sle, DMZ, PHSG SNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Glomerular Disease Types and PresentationsDocument58 pagesGlomerular Disease Types and PresentationsJosa Anggi Pratama0% (1)
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- HivDocument36 pagesHivfenendriyaniNo ratings yet
- PATH - Acute Kidney InjuryDocument12 pagesPATH - Acute Kidney InjuryAyyaz HussainNo ratings yet
- 5.nephritic SyndromeDocument64 pages5.nephritic Syndromeyeni100% (1)
- PECOMADocument25 pagesPECOMAAnan JaiswalNo ratings yet
- Von Willibrand DiseasesDocument34 pagesVon Willibrand DiseasesZulfadli Hussein100% (1)
- Sickle Cell Anemia - 27Document42 pagesSickle Cell Anemia - 27M.AhmedNo ratings yet
- Systemic Lupus ErythematosusDocument31 pagesSystemic Lupus ErythematosusJerilee SoCute WattsNo ratings yet
- Haematological DisordersDocument28 pagesHaematological DisordersSamuel kuriaNo ratings yet
- Infective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiDocument50 pagesInfective Endocarditis: Ainal Fadly Adigama PF Enny SuryantiFaisal Reza AdiebNo ratings yet
- Aplastic AnaemiaDocument21 pagesAplastic AnaemiaAbhinav ReddyNo ratings yet
- Rheumatic Fever and Rheumatic Heart Disease 2017 and IeDocument59 pagesRheumatic Fever and Rheumatic Heart Disease 2017 and IeLipi GautamNo ratings yet
- WBC Lymph Node SpleenDocument12 pagesWBC Lymph Node Spleendr brijesh TiwariNo ratings yet
- Rapidly Progressive Glomerulonephritis (RPGN): Causes, Symptoms, DiagnosisDocument13 pagesRapidly Progressive Glomerulonephritis (RPGN): Causes, Symptoms, DiagnosisArun GeorgeNo ratings yet
- Vasculitis: Ameen Kabaha, MD Wolfson Medical CenterDocument68 pagesVasculitis: Ameen Kabaha, MD Wolfson Medical Centeranaskabaha100% (1)
- Robbin's Chapter 20 Kidney PathologyDocument4 pagesRobbin's Chapter 20 Kidney Pathologynbaumgartner0100% (1)
- Blood - 6 (Anemia)Document9 pagesBlood - 6 (Anemia)drusmansaleemNo ratings yet
- WBC Pathology: Lecturer: Associate Professor T. A. GrekovaDocument49 pagesWBC Pathology: Lecturer: Associate Professor T. A. GrekovaFaheem MusthafaNo ratings yet
- Rapidly Progressive Glomerulonephritis - P. Devarajan PDFDocument48 pagesRapidly Progressive Glomerulonephritis - P. Devarajan PDFHerman HermanNo ratings yet
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Myeloproliferative Disorders (MPD) : Pathogenesis Clinical Laboratory FindingsDocument2 pagesMyeloproliferative Disorders (MPD) : Pathogenesis Clinical Laboratory FindingskakuNo ratings yet
- Microcytic Hypochromic Macrocytic Normochromic Normocytic: Anemia HematocritDocument7 pagesMicrocytic Hypochromic Macrocytic Normochromic Normocytic: Anemia Hematocritjjjj31No ratings yet
- Hafizuddin Mohamed Fauzi P-UM0037/10Document54 pagesHafizuddin Mohamed Fauzi P-UM0037/10Hafizuddin Mohamed FauziNo ratings yet
- Glomerular Diseases and Pathogenesis of Kidney InflammationDocument22 pagesGlomerular Diseases and Pathogenesis of Kidney InflammationrizapuspairyaniNo ratings yet
- Thalassemia & Bleeding DisordersDocument24 pagesThalassemia & Bleeding DisordersAbdulMushibNo ratings yet
- 19 Intro To AnemiaDocument3 pages19 Intro To AnemiaPeter JosephNo ratings yet
- Hematology - PathophysiologyDocument28 pagesHematology - Pathophysiologyjmosser100% (2)
- LupusDocument28 pagesLupusRiin IrasustaNo ratings yet
- Wilson S DiseaseDocument28 pagesWilson S DiseasemichaelcylNo ratings yet
- SleDocument66 pagesSleNur Liyana Ahmad Zaki100% (1)
- PBL Haematology (Bleeding) - B5Document49 pagesPBL Haematology (Bleeding) - B5nishibuchiNo ratings yet
- Glomerular DiseaseDocument18 pagesGlomerular DiseaseironNo ratings yet
- Myeloproliferative Diseases 2020Document105 pagesMyeloproliferative Diseases 2020Marc FosterNo ratings yet
- Pathology of Urinary SystemDocument384 pagesPathology of Urinary SystemNzau MuangeNo ratings yet
- GlomerulonephritisDocument59 pagesGlomerulonephritistressNo ratings yet
- Diseases of ImmunityDocument13 pagesDiseases of ImmunityRose AnnNo ratings yet
- The man who wins is the man who thinks he canDocument51 pagesThe man who wins is the man who thinks he cankays30002403No ratings yet
- Lecture 10 - Hemolytic Anemias - Extracorpuscular DefectsDocument28 pagesLecture 10 - Hemolytic Anemias - Extracorpuscular DefectsArif MaulanaNo ratings yet
- Ascites Hrs B WPDocument101 pagesAscites Hrs B WPGhias Un Nabi TayyabNo ratings yet
- Week 7. Renal Pathology Continued.Document9 pagesWeek 7. Renal Pathology Continued.Amber LeJeuneNo ratings yet
- Pathology - Chapter 4Document9 pagesPathology - Chapter 4Cory GrayNo ratings yet
- Vasculitic Disorders: Dra. MezaDocument47 pagesVasculitic Disorders: Dra. MezaAna Beatriz Meza OntiverosNo ratings yet
- Primary Immunodeficiency DiseasesDocument24 pagesPrimary Immunodeficiency DiseasesClaire Henderson100% (1)
- HematuriaDocument19 pagesHematuriaNycoNo ratings yet
- Liver Cirrhosis: Causes, Complications and ManagementDocument55 pagesLiver Cirrhosis: Causes, Complications and ManagementAnonymous vUEDx8100% (1)
- Hivan Ucla PDFDocument29 pagesHivan Ucla PDFAndrés David Calles UrdanetaNo ratings yet
- Acute GlomerulonephritisDocument27 pagesAcute GlomerulonephritisKumara GuruNo ratings yet
- Inflammation CCDocument72 pagesInflammation CCmulatumeleseNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemNo ratings yet
- Anti GBM DiseaseDocument36 pagesAnti GBM DiseaseHemanth PrakashNo ratings yet
- MDSDocument46 pagesMDSFesti Mada HelmiNo ratings yet
- Gastrointestinal PathologyDocument14 pagesGastrointestinal PathologyRahul ShuklaNo ratings yet
- PANCYTOPENIADocument51 pagesPANCYTOPENIAResmyNo ratings yet
- Anemia of Chronic Disorders (ACD)Document14 pagesAnemia of Chronic Disorders (ACD)Muhamad SyaifulNo ratings yet
- Kidney: Biochemical Tests For Assessing Renal FunctionsDocument56 pagesKidney: Biochemical Tests For Assessing Renal FunctionsPaulina Paskeviciute100% (1)
- Understanding Glomerular Diseases: Nephritic vs Nephrotic SyndromesDocument127 pagesUnderstanding Glomerular Diseases: Nephritic vs Nephrotic SyndromesCoy NuñezNo ratings yet
- Quarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierDocument2 pagesQuarterly Report On The Results of Treatment of Patients Registered 12-15 Months EarlierTrishenth FonsekaNo ratings yet
- Quarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseDocument1 pageQuarterly Report On Sputum Conversion of Positive Patients at The End of Intensive PhaseTrishenth FonsekaNo ratings yet
- Quarterly Report On Microscopic Activities and LogisticsDocument2 pagesQuarterly Report On Microscopic Activities and LogisticsTrishenth FonsekaNo ratings yet
- Quarterly Report On Case FindingDocument2 pagesQuarterly Report On Case FindingTrishenth FonsekaNo ratings yet
- Quarterly Report On Program ManagementDocument7 pagesQuarterly Report On Program ManagementTrishenth FonsekaNo ratings yet
- Laborotory Manual For Tuberculosis ControlDocument5 pagesLaborotory Manual For Tuberculosis ControlTrishenth FonsekaNo ratings yet
- Register of TB SuspectsDocument1 pageRegister of TB SuspectsTrishenth FonsekaNo ratings yet
- Quarterly Report On TB and non-TB WardsDocument3 pagesQuarterly Report On TB and non-TB WardsTrishenth FonsekaNo ratings yet
- National TB Control ManualDocument223 pagesNational TB Control ManualTrishenth FonsekaNo ratings yet
- The Premature BabyDocument92 pagesThe Premature BabyTrishenth Fonseka100% (1)
- National TB RegisterDocument2 pagesNational TB RegisterTrishenth FonsekaNo ratings yet
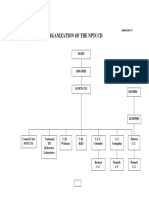
- Organization of NPTCCD PDFDocument2 pagesOrganization of NPTCCD PDFTrishenth FonsekaNo ratings yet
- Lab Form For Sputum Examination PDFDocument1 pageLab Form For Sputum Examination PDFTrishenth FonsekaNo ratings yet
- Duties of MOHDocument3 pagesDuties of MOHTrishenth FonsekaNo ratings yet
- QuotesDocument1 pageQuotesTrishenth FonsekaNo ratings yet
- Living With AFib Patient GuideDocument73 pagesLiving With AFib Patient GuideTrishenth FonsekaNo ratings yet
- 29 - Heart Disease Complicating PregnancyDocument18 pages29 - Heart Disease Complicating PregnancyTrishenth FonsekaNo ratings yet
- SLMC - Regulating Sri Lanka's Medical ProfessionDocument27 pagesSLMC - Regulating Sri Lanka's Medical ProfessionTrishenth FonsekaNo ratings yet
- Paediatric UrologyDocument194 pagesPaediatric UrologyTrishenth FonsekaNo ratings yet
- Gas Poisoning (Irrespirable Gases) : Asphyxial DeathDocument5 pagesGas Poisoning (Irrespirable Gases) : Asphyxial DeathTrishenth FonsekaNo ratings yet
- 15 - CN Poisoning 2Document2 pages15 - CN Poisoning 2Trishenth FonsekaNo ratings yet
- Neck Pain and Pain Down The ArmDocument27 pagesNeck Pain and Pain Down The ArmTrishenth FonsekaNo ratings yet
- 11 - Professional SecrecyDocument10 pages11 - Professional SecrecyTrishenth Fonseka100% (1)
- 13 - Medicolegal Duties of A DoctorDocument13 pages13 - Medicolegal Duties of A DoctorTrishenth FonsekaNo ratings yet
- Medical Ethics Code ExplainedDocument23 pagesMedical Ethics Code ExplainedTrishenth FonsekaNo ratings yet
- 12 - Medical NegligenceDocument34 pages12 - Medical NegligenceTrishenth FonsekaNo ratings yet
- 10 - Introduction To Legal System in SLDocument6 pages10 - Introduction To Legal System in SLTrishenth FonsekaNo ratings yet
- 09 - Changes After Death and Time Since DeathDocument9 pages09 - Changes After Death and Time Since DeathTrishenth FonsekaNo ratings yet
- 08 - Post Mortem InstrumentsDocument6 pages08 - Post Mortem InstrumentsTrishenth FonsekaNo ratings yet
- Microbiology and Parasitology Recall QuestionsDocument3 pagesMicrobiology and Parasitology Recall QuestionsKenneth MiguelNo ratings yet
- 2018 - Guardian Life Claim FormDocument2 pages2018 - Guardian Life Claim FormSherene Boochoon60% (5)
- Healthmedicinet I 2016 2Document290 pagesHealthmedicinet I 2016 2tuni santeNo ratings yet
- Albumin Piggyback Procedure ChecklistDocument3 pagesAlbumin Piggyback Procedure ChecklistAljane VistoNo ratings yet
- Rapid 12-Lead ECG and Capnography Interpretation WorkshopDocument1 pageRapid 12-Lead ECG and Capnography Interpretation WorkshopMohammad Usman QureshiNo ratings yet
- Assisted Deliveries CertificationDocument2 pagesAssisted Deliveries Certificationapi-3747282No ratings yet
- CABG - On Pump Vs Off Pump - AHA 2005Document7 pagesCABG - On Pump Vs Off Pump - AHA 2005odiseu81No ratings yet
- Phil Callahan - An Interview With Joe BlankenshipDocument139 pagesPhil Callahan - An Interview With Joe Blankenshipselenite plus100% (2)
- Challenges To Implementation of The Pharmaceutical Care Practice in Davao City.Document11 pagesChallenges To Implementation of The Pharmaceutical Care Practice in Davao City.JessieLynMolinaNo ratings yet
- Forensic MedicineDocument9 pagesForensic Medicinev_vijayakanth7656No ratings yet
- H2o2 Xprogram H2o2 Program Vodikov Peroksid Za KonzumiranjeDocument2 pagesH2o2 Xprogram H2o2 Program Vodikov Peroksid Za Konzumiranjespajk6No ratings yet
- Topic 2-Production of Radionuclides & QA QCDocument62 pagesTopic 2-Production of Radionuclides & QA QCEdwin MccainNo ratings yet
- Modern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDDocument21 pagesModern Management of Cardiogenic Pulmonary Edema: Amal Mattu, MD, Joseph P. Martinez, MD, Brian S. Kelly, MDJoni MokodoNo ratings yet
- Use of Animals in Product DevelopmentDocument4 pagesUse of Animals in Product DevelopmentMerih SunNo ratings yet
- Basic ECG Interpretation Practice Test: DIRECTIONS: The Following Test Consists of 20 QuestionsDocument10 pagesBasic ECG Interpretation Practice Test: DIRECTIONS: The Following Test Consists of 20 Questionsmihaela_bondocNo ratings yet
- Medical Certificate For AthletesDocument2 pagesMedical Certificate For AthletesCaitlin PeñeraNo ratings yet
- Pharma Midterms Review UwuDocument11 pagesPharma Midterms Review UwuAJ BayNo ratings yet
- Health Education Plan-DiarrheaDocument10 pagesHealth Education Plan-DiarrheaMae Dacer50% (2)
- Induction Training Program For Newly Recruited NursesDocument17 pagesInduction Training Program For Newly Recruited NursesNisha sutariyaNo ratings yet
- General Directory Site: Walter C. Mackenzie Health Sciences CentreDocument1 pageGeneral Directory Site: Walter C. Mackenzie Health Sciences CentreAli MullaNo ratings yet
- Interocclusal RecordsDocument8 pagesInterocclusal RecordsJohnNo ratings yet
- DelegatesDocument11 pagesDelegatesVikrant Tomar0% (1)
- Depression Powerpoint - 2Document26 pagesDepression Powerpoint - 2danyalNo ratings yet
- Contoh Layout PabrikDocument1 pageContoh Layout PabrikArikMochamadNo ratings yet
- Kate Laver's Primary FRCA Guide: My Revision (For Exam in June)Document3 pagesKate Laver's Primary FRCA Guide: My Revision (For Exam in June)M H DuNo ratings yet
- Medical Terminology TermsDocument28 pagesMedical Terminology TermsNikka Moreen DagdagNo ratings yet
- Case Study of PIMSDocument35 pagesCase Study of PIMSMandeep Bhatia50% (2)
- Pediatric Fever, Cough and Rash ExamDocument3 pagesPediatric Fever, Cough and Rash ExamTheju ReddyNo ratings yet
- DrugDocument4 pagesDrugApril Daye B. AsuncionNo ratings yet
- Ef310 Unit 8 Carls Assessment Part 2Document3 pagesEf310 Unit 8 Carls Assessment Part 2api-473700764No ratings yet