You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
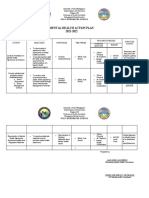
- Mental Health Action PlanDocument2 pagesMental Health Action PlanKenny Ann Grace Batiancila100% (9)
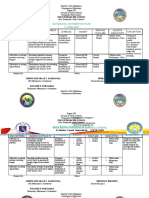
- Guidance and Counseling Action Plan (2022-2023)Document3 pagesGuidance and Counseling Action Plan (2022-2023)Kenny Ann Grace Batiancila100% (2)
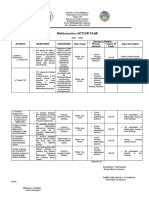
- Math 9 (Cot 1)Document5 pagesMath 9 (Cot 1)Kenny Ann Grace Batiancila100% (1)
- MATH Action Plan (2022 2023)Document3 pagesMATH Action Plan (2022 2023)Kenny Ann Grace Batiancila100% (5)
- Certificate 2022-2023Document11 pagesCertificate 2022-2023Kenny Ann Grace BatiancilaNo ratings yet
- Mental Health Action Plan 2022-2023Document2 pagesMental Health Action Plan 2022-2023Kenny Ann Grace Batiancila100% (6)
- Screening Test, Grade 7Document26 pagesScreening Test, Grade 7Kenny Ann Grace BatiancilaNo ratings yet
- Certificate For StakeholdersDocument1 pageCertificate For StakeholdersKenny Ann Grace Batiancila100% (1)
- Math Intervention Plan Docx 1Document6 pagesMath Intervention Plan Docx 1Kenny Ann Grace BatiancilaNo ratings yet
- Award Certificates For StudentsDocument4 pagesAward Certificates For StudentsKenny Ann Grace BatiancilaNo ratings yet
- Certificate As HostDocument5 pagesCertificate As HostKenny Ann Grace BatiancilaNo ratings yet
- AGE SEX Grade Section School YearDocument12 pagesAGE SEX Grade Section School YearKenny Ann Grace BatiancilaNo ratings yet
- Certificate of CommendationDocument4 pagesCertificate of CommendationKenny Ann Grace BatiancilaNo ratings yet
- District CertificationDocument4 pagesDistrict CertificationKenny Ann Grace BatiancilaNo ratings yet
- MATH Action Plan New NormalDocument2 pagesMATH Action Plan New NormalKenny Ann Grace BatiancilaNo ratings yet
- Certificate of Recognition: PO3 Rocel Yn D. HolleDocument11 pagesCertificate of Recognition: PO3 Rocel Yn D. HolleKenny Ann Grace BatiancilaNo ratings yet
- Guidance and Counseling Action Plan (2021-2022)Document2 pagesGuidance and Counseling Action Plan (2021-2022)Kenny Ann Grace Batiancila100% (2)
- Certificate of RecognitionDocument12 pagesCertificate of RecognitionKenny Ann Grace BatiancilaNo ratings yet
- Tos Mathematics 7 q3Document2 pagesTos Mathematics 7 q3Kenny Ann Grace Batiancila100% (1)
- Polo Integrated School Third Periodical Exam in Mathematics 7Document5 pagesPolo Integrated School Third Periodical Exam in Mathematics 7Kenny Ann Grace BatiancilaNo ratings yet
- Tos - Mapeh 8 - Q2Document2 pagesTos - Mapeh 8 - Q2Kenny Ann Grace BatiancilaNo ratings yet
- Group Synergy in Problem SolvingDocument29 pagesGroup Synergy in Problem SolvingKenny Ann Grace BatiancilaNo ratings yet
- Mathematics Action Plan 2021-2022: Polo Integrated SchoolDocument3 pagesMathematics Action Plan 2021-2022: Polo Integrated SchoolKenny Ann Grace BatiancilaNo ratings yet
- Resource Allocation and Mobilization PlanDocument4 pagesResource Allocation and Mobilization PlanKenny Ann Grace BatiancilaNo ratings yet
- Parenting SeminarDocument27 pagesParenting SeminarKenny Ann Grace Batiancila100% (1)
- Health 8 Module 2Document21 pagesHealth 8 Module 2Kenny Ann Grace Batiancila100% (6)
- SBM Scoring Matrix Validation Form: Step 1: Determine Performance Improvement (60%)Document29 pagesSBM Scoring Matrix Validation Form: Step 1: Determine Performance Improvement (60%)Kenny Ann Grace BatiancilaNo ratings yet
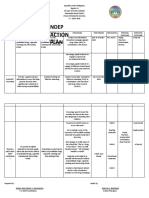
- Ndep Action Plan: Polo Integrated SchoolDocument2 pagesNdep Action Plan: Polo Integrated SchoolKenny Ann Grace Batiancila100% (3)
- ProjectsDocument3 pagesProjectsJoy DasNo ratings yet
- Technical Assesment Form-Invisa SkyDocument5 pagesTechnical Assesment Form-Invisa SkyGerald TashingaNo ratings yet
- Analysis of Systematic Investment Plan and Lump Sum InvestmentDocument6 pagesAnalysis of Systematic Investment Plan and Lump Sum InvestmentshanedsouzaNo ratings yet
- Application For Registration: Kawanihan NG Rentas InternasDocument4 pagesApplication For Registration: Kawanihan NG Rentas InternasCarl PedreraNo ratings yet
- Learning Outcome Based Vocational Curriculum: Job Role: Unarmed Security GuardDocument39 pagesLearning Outcome Based Vocational Curriculum: Job Role: Unarmed Security GuardSHIELD PLUS ARMORNo ratings yet
- BBA 2003 Cost AccountingDocument24 pagesBBA 2003 Cost AccountingVentus TanNo ratings yet
- Worksheet About Breakeven AnalysisDocument2 pagesWorksheet About Breakeven AnalysisAnuka YituNo ratings yet
- Elisas Crochet Sheep Crochet PatternDocument3 pagesElisas Crochet Sheep Crochet PatternantiFlash100% (2)
- Teacher Efficacy Research 1998 - 2009: Signs of Progress or Unfulfilled Promise?Document24 pagesTeacher Efficacy Research 1998 - 2009: Signs of Progress or Unfulfilled Promise?Dorin TriffNo ratings yet
- A Systematic ReviewDocument24 pagesA Systematic ReviewChris KotchieNo ratings yet
- Conservation of Architectural Ironwork - Decay Mechanisms and Hazards by David MitchellDocument13 pagesConservation of Architectural Ironwork - Decay Mechanisms and Hazards by David MitchellDebashrita KunduNo ratings yet
- Everything Is DolphinsDocument43 pagesEverything Is DolphinsDingusbubmisNo ratings yet
- The Hawthorne Studies and Human RelationsDocument2 pagesThe Hawthorne Studies and Human Relationsarief2cNo ratings yet
- Electronic EngineerDocument2 pagesElectronic EngineernomimanNo ratings yet
- Hardox 450: General Product DescriptionDocument2 pagesHardox 450: General Product DescriptionTeodor EzaruNo ratings yet
- Archives Search Report September 1993Document571 pagesArchives Search Report September 1993FrancescoNo ratings yet
- Screenshot 2021-09-20 at 6.22.14 PMDocument1 pageScreenshot 2021-09-20 at 6.22.14 PMAsim KhanNo ratings yet
- Last Christmas - WhamDocument3 pagesLast Christmas - Whamnicograuby100% (2)
- Russell's Criticism of Logical PositivismDocument33 pagesRussell's Criticism of Logical PositivismDoda BalochNo ratings yet
- Tech Questions in InterviewDocument176 pagesTech Questions in InterviewGajarajakrishnan JanarthanamNo ratings yet
- Instant Download Test Bank For Gender Psychological Perspectives 7th Edition Brannon PDF EbookDocument32 pagesInstant Download Test Bank For Gender Psychological Perspectives 7th Edition Brannon PDF EbookAmos Kerr100% (16)
- Enuma Anu EnlilDocument10 pagesEnuma Anu EnlilPron Goes100% (3)
- Glazing and Curtain Wall Prices Philippines - PHILCON PRICESDocument1 pageGlazing and Curtain Wall Prices Philippines - PHILCON PRICESjohn reyesNo ratings yet
- CBI Class Reads Level 1Document30 pagesCBI Class Reads Level 1Arildo LealNo ratings yet
- Ac115 Ac165Document84 pagesAc115 Ac165The WorkshopNo ratings yet
- CHAPTER 3 and 4Document12 pagesCHAPTER 3 and 4albert matandagNo ratings yet
- Nessus 3.0 Installation GuideDocument63 pagesNessus 3.0 Installation GuideLovely GreenNo ratings yet
- Commissioner Rebecca Benally Speech On Bears Ears, Edits by Sutherland InstituteDocument4 pagesCommissioner Rebecca Benally Speech On Bears Ears, Edits by Sutherland InstituteThe Salt Lake TribuneNo ratings yet
- Problems On Sole PropritersDocument10 pagesProblems On Sole PropritersMouly ChopraNo ratings yet
- GenBio Q2 M1Document16 pagesGenBio Q2 M1Allaine BenitezNo ratings yet