You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Tao of Revitalization: Exercises For Self-HealingDocument25 pagesTao of Revitalization: Exercises For Self-HealingAnirudh100% (1)
- Partus Immaturus, Prematurus, Serotinus.: Dr. Fery Kusnadi, SpogDocument60 pagesPartus Immaturus, Prematurus, Serotinus.: Dr. Fery Kusnadi, SpogArtika MayandaNo ratings yet
- Kelainan Pada Sistem Saraf PeriferDocument144 pagesKelainan Pada Sistem Saraf PeriferArtika MayandaNo ratings yet
- Farmakologi OpioidDocument24 pagesFarmakologi OpioidArtika MayandaNo ratings yet
- Thoracic Trauma: Clinical Science SessionDocument31 pagesThoracic Trauma: Clinical Science SessionArtika MayandaNo ratings yet
- ECG Rythum Study Guide PDFDocument9 pagesECG Rythum Study Guide PDFArtika MayandaNo ratings yet
- Surgical DressingDocument2 pagesSurgical Dressinggao1989No ratings yet
- Comparison Chart BlsDocument2 pagesComparison Chart BlsjeffNo ratings yet
- PediahandynotesDocument62 pagesPediahandynotesEduardo AnerdezNo ratings yet
- L01 Obs. - History - Dr.a.rahim 2021 2022Document5 pagesL01 Obs. - History - Dr.a.rahim 2021 2022salmaNo ratings yet
- Science and Health Writing MaterialDocument2 pagesScience and Health Writing MaterialMora, Aileen Joy R.100% (1)
- Genitourinary Emergency: Prof. Dr. Mostafa Sakr Genitourinary SurgeryDocument83 pagesGenitourinary Emergency: Prof. Dr. Mostafa Sakr Genitourinary SurgeryKeserovic AdmirNo ratings yet
- 0000 Septodont UK Pain Control Red and WhiteDocument7 pages0000 Septodont UK Pain Control Red and WhiteBryant LewisNo ratings yet
- Dosages: Treatment of Influenza and Other DiseasesDocument6 pagesDosages: Treatment of Influenza and Other Diseasesmartdot73490100% (8)
- Michael John R. Aguilar, RMTDocument41 pagesMichael John R. Aguilar, RMTFrankenstein MelancholyNo ratings yet
- Blood Collection GuidelinesDocument10 pagesBlood Collection GuidelinesyechezkielNo ratings yet
- Anterior Cruciate Ligament All InsideDocument7 pagesAnterior Cruciate Ligament All InsideVijay KumarNo ratings yet
- IFU For Bone Plate Locking Plate Bone Screw Locking ScrewPin WireMaxillofacial ImplantDocument6 pagesIFU For Bone Plate Locking Plate Bone Screw Locking ScrewPin WireMaxillofacial ImplantErRajeshNo ratings yet
- Nursing Care Plan For Acute BronchitisDocument6 pagesNursing Care Plan For Acute BronchitisNur Panca Retnaningsih50% (2)
- Suturing - OxfordDocument12 pagesSuturing - OxfordGhada Al-OgailyNo ratings yet
- Management of Health Equipment Clinic Medical Center Public Universities in East JavaDocument12 pagesManagement of Health Equipment Clinic Medical Center Public Universities in East JavaIlham SandegiNo ratings yet
- Pelvic Examination: Uses, Procedure, ResultsDocument11 pagesPelvic Examination: Uses, Procedure, ResultsnamanNo ratings yet
- Clinicopathological Correlation in Diagnosis of Hansen's Disease: A Histopathologist's PerspectiveDocument12 pagesClinicopathological Correlation in Diagnosis of Hansen's Disease: A Histopathologist's PerspectiveRani Dwi HapsariNo ratings yet
- Arterial Blood Gases - UpToDateDocument13 pagesArterial Blood Gases - UpToDatedevi efrinaNo ratings yet
- Evaluasi Program Early Warning Alert and Surveilans KLB Kota Salatiga Provinsi Jawa TengahDocument9 pagesEvaluasi Program Early Warning Alert and Surveilans KLB Kota Salatiga Provinsi Jawa TengahIinAstikaNo ratings yet
- Female Medical Undergraduate : Does Marriage Affect The Academic Performance in A Saudi University?Document4 pagesFemale Medical Undergraduate : Does Marriage Affect The Academic Performance in A Saudi University?Ali AlomyNo ratings yet
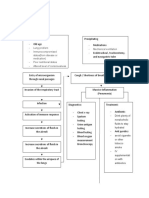
- Pathophysiology PneumoniaDocument2 pagesPathophysiology PneumoniaChiro Rouy Malaluan100% (2)
- A Rare Case of Hereditary Sensory and Autonomic Neuropathy Type IIDocument4 pagesA Rare Case of Hereditary Sensory and Autonomic Neuropathy Type IITalbiya mullaNo ratings yet
- Sexuality Research in India An UpdateDocument5 pagesSexuality Research in India An UpdatekavalapparaNo ratings yet
- Research Brochure PDFDocument30 pagesResearch Brochure PDFRajkumar ANo ratings yet
- Anticancer Plant-Derivatives: Deciphering Their Oncopreventive and Therapeutic Potential in Molecular TermsDocument30 pagesAnticancer Plant-Derivatives: Deciphering Their Oncopreventive and Therapeutic Potential in Molecular Termsbmounika 206No ratings yet
- What Is RH Sensitization During PregnancyDocument14 pagesWhat Is RH Sensitization During PregnancyKeisha Ferreze Ann QuiñonesNo ratings yet
- RUHS Pre D.M.medical Gastroenterology Entrance Exam Question Paper 2014Document17 pagesRUHS Pre D.M.medical Gastroenterology Entrance Exam Question Paper 2014narasimhahanNo ratings yet
- NCP Rheumatoid ArthritisDocument2 pagesNCP Rheumatoid ArthritisPatty RomeroNo ratings yet
- TMJ Postgraduate ProgramDocument8 pagesTMJ Postgraduate ProgramsorcNo ratings yet