You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Epsilon EP 500 - Medicare Xray MachineDocument10 pagesEpsilon EP 500 - Medicare Xray MachineJoseph SsaliNo ratings yet
- Presentation On: 2 X 25 KV SystemDocument28 pagesPresentation On: 2 X 25 KV SystemAkhilesh kumar Srivastava100% (4)
- Innovative Rail Fastening SystemsDocument9 pagesInnovative Rail Fastening SystemsShahryarNo ratings yet
- Kochi RailwayDocument38 pagesKochi RailwayMOUNIKA PURETI VP21ARCH0100010No ratings yet
- Detailed Design Stage ChecklistDocument17 pagesDetailed Design Stage ChecklistCzar RosuelloNo ratings yet
- CAE QuestionsDocument1 pageCAE QuestionsanajamaicaNo ratings yet
- EstacionesRepetidoras Al 01.03.2023Document15 pagesEstacionesRepetidoras Al 01.03.2023Victor Daniel LopezNo ratings yet
- D143 Briones Research Proposal PrelimDocument28 pagesD143 Briones Research Proposal PrelimRicojohn ManimtimNo ratings yet
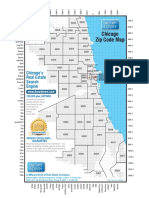
- Chicago Zipcode Map PDFDocument1 pageChicago Zipcode Map PDFAftab AjmeriNo ratings yet
- E Project09 FullDocument137 pagesE Project09 Fullરામ પ્રતાપNo ratings yet
- Iriset: S2 Principles of Interlocking Electro-Mechanical Inter Locking CircuitsDocument93 pagesIriset: S2 Principles of Interlocking Electro-Mechanical Inter Locking CircuitsRavi NikilNo ratings yet
- New Lakewood ScheduleDocument1 pageNew Lakewood ScheduleLupita PortilloNo ratings yet
- Autonomous Tram by SiemensDocument2 pagesAutonomous Tram by SiemenskssekharNo ratings yet
- Chapter 5 Generator TransformerDocument27 pagesChapter 5 Generator TransformerAnonymous nwByj9LNo ratings yet
- Means of Transport Elementary WorksheetDocument14 pagesMeans of Transport Elementary WorksheetOtilia SîrbuNo ratings yet
- TSSPDCL, Operation Circle: Mahabubnagar: Description Designation Cell NoDocument1 pageTSSPDCL, Operation Circle: Mahabubnagar: Description Designation Cell NoShyam Sunder Rao KandukuriNo ratings yet
- Prefabrication of Tunnel Elements On The Oresund TunnelDocument14 pagesPrefabrication of Tunnel Elements On The Oresund Tunnelilyas16No ratings yet
- Container Is at IonDocument29 pagesContainer Is at IonAbi JamesNo ratings yet
- A Developed Country Is Not A Place Where The Poor Have CarsDocument3 pagesA Developed Country Is Not A Place Where The Poor Have Carsderpyherpy derpyNo ratings yet
- Report On Bridge Development in PakistanDocument8 pagesReport On Bridge Development in Pakistankhawaja Ali100% (1)
- Budapest GuideDocument100 pagesBudapest Guideuivar09No ratings yet
- 06-07 Ladder Slides Down The Wall - Differential Calculus ReviewDocument4 pages06-07 Ladder Slides Down The Wall - Differential Calculus ReviewJayson J. PagalNo ratings yet
- Railway Stations SpecsDocument288 pagesRailway Stations SpecsFranklin GarciaNo ratings yet
- Peri MULTIPROP PDFDocument28 pagesPeri MULTIPROP PDFboctraian55No ratings yet
- 5 Transportation System: Learning ObjectiveDocument20 pages5 Transportation System: Learning ObjectiveGh LimNo ratings yet
- Train ScheduleDocument2 pagesTrain ScheduleAsad ZamanNo ratings yet
- TGN 08 Crane Rail Selection 2Document3 pagesTGN 08 Crane Rail Selection 2Prasad PatilNo ratings yet
- Thomson Roundrail 2DA Modular SpecsheetDocument2 pagesThomson Roundrail 2DA Modular SpecsheetElectromateNo ratings yet
- 400-Eng-9336-003 Rev 00 (Technical Specification For 220KV Switchyard) PDFDocument69 pages400-Eng-9336-003 Rev 00 (Technical Specification For 220KV Switchyard) PDFSridhar Reddy Gandra100% (1)
- Nagoya and VicinityDocument5 pagesNagoya and VicinitymandalsoumyaNo ratings yet