You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Glasgow Coma Scale: Presented by Pankaj Singh Rana Nurse Practitioner in Critical CareDocument17 pagesGlasgow Coma Scale: Presented by Pankaj Singh Rana Nurse Practitioner in Critical CareAnisya AbabeliaNo ratings yet
- 18 Carpal Bone FracturesDocument69 pages18 Carpal Bone FracturesAdina BotezNo ratings yet
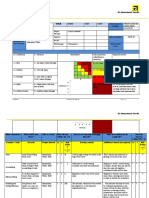
- Risk Assessment - Aluminium WorksDocument4 pagesRisk Assessment - Aluminium Worksburak0% (1)
- MortonDocument1 pageMortonAdina BotezNo ratings yet
- House Cleaning Checklist PDFDocument1 pageHouse Cleaning Checklist PDFAdina Botez100% (1)
- RizartrozaDocument3 pagesRizartrozaAdina BotezNo ratings yet
- Carpal Tunnel - Merten (Seminar)Document14 pagesCarpal Tunnel - Merten (Seminar)Adina BotezNo ratings yet
- Examenul Clinic Al MainiiDocument33 pagesExamenul Clinic Al MainiiAdina Botez100% (2)
- Article: Cost-Effectiveness of Colonoscopy in Screening For Colorectal CancerDocument12 pagesArticle: Cost-Effectiveness of Colonoscopy in Screening For Colorectal CancerAdina BotezNo ratings yet
- Passive ImmunizationDocument1 pagePassive ImmunizationAdina BotezNo ratings yet
- Nerves of Upper LimbDocument13 pagesNerves of Upper LimbHafiz NaveedNo ratings yet
- CPR/AED/First Aid TrainingDocument50 pagesCPR/AED/First Aid TrainingThe Health Therapist AcademyNo ratings yet
- Wheelchairs 1Document72 pagesWheelchairs 1Dr. JDPNo ratings yet
- Fractured Thumb 5Document20 pagesFractured Thumb 5Noor Al Zahraa AliNo ratings yet
- Syndesmosis: Ankle Ligament IntroductionDocument4 pagesSyndesmosis: Ankle Ligament Introductionkajal sharmaNo ratings yet
- Compendium 2014 PDFDocument47 pagesCompendium 2014 PDFadidaya100% (5)
- 01 Introductory PgyDocument76 pages01 Introductory Pgygbsreg gbsregNo ratings yet
- Ing 4 SNBT 2023 PDFDocument4 pagesIng 4 SNBT 2023 PDFjenniferNo ratings yet
- Mark Dutton - Manual Therapy of The Spine - An Integrated Approach-Appleton & Lange (2001)Document626 pagesMark Dutton - Manual Therapy of The Spine - An Integrated Approach-Appleton & Lange (2001)Suhani Mihai100% (1)
- Doc023 97 80087Document132 pagesDoc023 97 80087alejandra manjarresNo ratings yet
- Skeleton Printable GameDocument5 pagesSkeleton Printable GameRizki AmaliyahNo ratings yet
- Hand InfectionsDocument10 pagesHand InfectionsAhmed S. AlkhalifahNo ratings yet
- User Manual: Model 4779 Tru-Trac® Traction UnitDocument46 pagesUser Manual: Model 4779 Tru-Trac® Traction UnitSejmet IngenieriaNo ratings yet
- Eight Rules For The Haemodynamic Management of Traumatic Brain-Injured PatientsDocument9 pagesEight Rules For The Haemodynamic Management of Traumatic Brain-Injured PatientsBenjamínGalvanNo ratings yet
- Basic First Aid ExamDocument2 pagesBasic First Aid ExamEMS Region2No ratings yet
- Faradic Current: Prof - Dr. Mahmoud EwideaDocument75 pagesFaradic Current: Prof - Dr. Mahmoud EwideaMahi GuptaNo ratings yet
- Anatomy and Physiology of Tibia and FibulaDocument3 pagesAnatomy and Physiology of Tibia and FibulaVel Georgia-Franco50% (2)
- Ylarde vs. Aquino, GR 33722 (DIGEST)Document1 pageYlarde vs. Aquino, GR 33722 (DIGEST)Lourdes LorenNo ratings yet
- Massive Hemorrhage ProtocolDocument19 pagesMassive Hemorrhage ProtocolYeseniaNo ratings yet
- Wave RunnerDocument182 pagesWave RunnerclaudiovaldezNo ratings yet
- ReflexDocument2 pagesReflexSarah LewisNo ratings yet
- 5 HemophiliaDocument57 pages5 HemophiliaRabia AzharNo ratings yet
- Physical Examination Till October 2017Document15 pagesPhysical Examination Till October 2017qurbanNo ratings yet
- P E-ScriptDocument5 pagesP E-ScriptAnime LoverNo ratings yet
- MMM Ws BonyLandmarks HandDocument1 pageMMM Ws BonyLandmarks Handjmccoy26No ratings yet
- Effectiveness of Exercise Interventions To Prevent.16Document10 pagesEffectiveness of Exercise Interventions To Prevent.16rodrigo weyllNo ratings yet
- To This DayDocument5 pagesTo This Dayyuriana8aNo ratings yet
- Flexion: To Improve Movement of The PivotalDocument3 pagesFlexion: To Improve Movement of The PivotalKelsey MacaraigNo ratings yet