You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Pediatrics - Question Bank - RGUHSDocument51 pagesPediatrics - Question Bank - RGUHSArun Kumar88% (8)
- Challenging Cases in PaediatricsDocument569 pagesChallenging Cases in PaediatricsRebecca Wong100% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Case Study Celiac DiseaseDocument8 pagesCase Study Celiac Diseaseapi-242376719No ratings yet
- Crohn's DiseaseDocument46 pagesCrohn's Diseaseuttarasingh100% (3)
- SWL Vitamin D Guidelines For Adults and ChildrenDocument17 pagesSWL Vitamin D Guidelines For Adults and ChildrenKermicheNo ratings yet
- Characteristics of Stool 869Document10 pagesCharacteristics of Stool 869Divine IncilloNo ratings yet
- Michael Kaminski-Case 5Document7 pagesMichael Kaminski-Case 5api-302058832No ratings yet
- Malabsorption Syndromes in Children PDFDocument6 pagesMalabsorption Syndromes in Children PDFkoreswilsonNo ratings yet
- Nursing Care of Patients With Cancer: Maintaining Tissue IntegrityDocument5 pagesNursing Care of Patients With Cancer: Maintaining Tissue Integrityela garciaNo ratings yet
- Schilling TestDocument13 pagesSchilling TestLyn OdchigueNo ratings yet
- Pancreatic Function TestsDocument12 pagesPancreatic Function TestsDhera CharlesNo ratings yet
- NCP Vol 33 No 4Document120 pagesNCP Vol 33 No 4Marwah RifahNo ratings yet
- Urine Indican Excretion in Malabsorptive DisordersDocument8 pagesUrine Indican Excretion in Malabsorptive DisordersBiancake Sta. AnaNo ratings yet
- Chapter 33 The Child With Gastrointestinal DysfunctionDocument9 pagesChapter 33 The Child With Gastrointestinal DysfunctionKBNo ratings yet
- Nutrients 13 04337Document23 pagesNutrients 13 04337dr.martynchukNo ratings yet
- Malabsorption Syndrome Malaika NaseerDocument10 pagesMalabsorption Syndrome Malaika NaseerEntertainment MoviesNo ratings yet
- Strategies To Address Age-Related Changes Affecting NutritionDocument52 pagesStrategies To Address Age-Related Changes Affecting NutritionVictoriaNo ratings yet
- NutriDiet ReviewerDocument6 pagesNutriDiet ReviewerCherry BoticarioNo ratings yet
- Jurnal MalabsorbsiDocument6 pagesJurnal MalabsorbsiIda Putri IhsaniNo ratings yet
- Malabsorption SyndromeDocument7 pagesMalabsorption SyndromeHassan.shehri100% (4)
- Matarese2012 PDFDocument11 pagesMatarese2012 PDFYacine Tarik AizelNo ratings yet
- Stool Exam HandoutDocument5 pagesStool Exam HandoutAhmed GaberNo ratings yet
- Fat Malabsorption in Critical IllnessDocument6 pagesFat Malabsorption in Critical Illnesslakshminivas PingaliNo ratings yet
- Anemia Defisiensi Asam FolatDocument15 pagesAnemia Defisiensi Asam FolatKertiasihwayanNo ratings yet
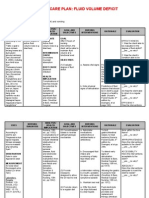
- NCP-Fluid Volume DeficitDocument2 pagesNCP-Fluid Volume Deficitjava_biscocho122979% (33)
- Extra-Intestinal and Long Term Consequences of GiardiaDocument13 pagesExtra-Intestinal and Long Term Consequences of GiardiaDulce Nalleli Aguilar TejedaNo ratings yet
- Celiac DiseaseDocument42 pagesCeliac DiseaseTri P BukerNo ratings yet
- Chronic Diarrhea and Malabsorption GssDocument50 pagesChronic Diarrhea and Malabsorption GssIPNATC NEPAL100% (1)
- Manajemen Diare AkutDocument24 pagesManajemen Diare Akutsawitri dewiNo ratings yet