You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
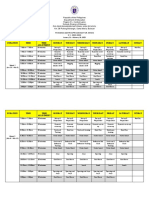
- Arnis Traning Matrix 2023Document6 pagesArnis Traning Matrix 2023RA CastroNo ratings yet
- Defranco'S Training - Ask Joe 07.18.03Document622 pagesDefranco'S Training - Ask Joe 07.18.03Alex23No ratings yet
- Unlocking Myofascial PadlocksDocument49 pagesUnlocking Myofascial PadlocksAnonymous FNJJSCB100% (8)
- Week 3 Different Types of StretchingDocument25 pagesWeek 3 Different Types of StretchingAyah Garcia100% (1)
- 4 Weeks To Total Posture & Spinal Mobility: Beginner - IntermediateDocument14 pages4 Weeks To Total Posture & Spinal Mobility: Beginner - Intermediate714 BaliNo ratings yet
- Flexibility Training: Len Kravitz, Ph.D. and Vivian H. Heyward, PH.DDocument12 pagesFlexibility Training: Len Kravitz, Ph.D. and Vivian H. Heyward, PH.Dgschiro100% (1)
- Instructional Module: Republic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaDocument7 pagesInstructional Module: Republic of The Philippines Nueva Vizcaya State University Bayombong, Nueva VizcayaAkemi YeonNo ratings yet
- Gcse Pe Revision BookletDocument36 pagesGcse Pe Revision Bookletharshi singhNo ratings yet
- Exercise For Fitness: "Strengthen Your Faith Through Physical Exercise"Document19 pagesExercise For Fitness: "Strengthen Your Faith Through Physical Exercise"Goodness- Gabihan, IyannaNo ratings yet
- PNF As A Training System (Siff)Document6 pagesPNF As A Training System (Siff)Tom FarrowNo ratings yet
- Finding Your Maximum Flexibility in YogaDocument10 pagesFinding Your Maximum Flexibility in Yogaadaminindia26No ratings yet
- General Exercise ConceptDocument43 pagesGeneral Exercise ConceptEisha KhanNo ratings yet
- 1st Day Physical EducationDocument13 pages1st Day Physical EducationEsmael KasilagNo ratings yet
- W 1 PE 2 MOdDocument9 pagesW 1 PE 2 MOdLynGirl YanezNo ratings yet
- Dynamic Warm-Up Exercises Instead of Traditional RoutinesDocument2 pagesDynamic Warm-Up Exercises Instead of Traditional RoutinespodamakriNo ratings yet
- Pe 11Document22 pagesPe 11Glaziel BenalayoNo ratings yet
- Stretching OldDocument5 pagesStretching OldGin CruzNo ratings yet
- Beginners Basic Bodyweight Program NEWDocument26 pagesBeginners Basic Bodyweight Program NEWStevanovic VladimirNo ratings yet
- The 12-Month Soccer Training ProgramDocument15 pagesThe 12-Month Soccer Training ProgramOttoman Edit100% (1)
- Pe 02 - Physical Education and Health 2 Learning Points Sheet Quarter 3 - Week 1 A Glimpse of Health Optimizing P.E. 1 (H.O.P.E. 1) IntroductionDocument10 pagesPe 02 - Physical Education and Health 2 Learning Points Sheet Quarter 3 - Week 1 A Glimpse of Health Optimizing P.E. 1 (H.O.P.E. 1) IntroductionAizel Joyce DomingoNo ratings yet
- Music - Arts - Physical Education - HealthDocument10 pagesMusic - Arts - Physical Education - HealthElbert NatalNo ratings yet
- SanchezJireme PE1 Final AssignmentDocument19 pagesSanchezJireme PE1 Final AssignmentJireme SanchezNo ratings yet
- Intermediate Sprint Training ProgramDocument40 pagesIntermediate Sprint Training ProgramLebonolo “Lo” ThimotheusNo ratings yet
- Splits Guide Top ExercisesDocument16 pagesSplits Guide Top ExercisesBorivoje Stojiljkovic100% (1)
- Cambridge Assessment International Education: Physical Education 9396/33 October/November 2019Document10 pagesCambridge Assessment International Education: Physical Education 9396/33 October/November 2019Carlos GallardoNo ratings yet
- 1ST Hope 1Document5 pages1ST Hope 1Jayson RigorNo ratings yet
- Basic Gymnastics: Tarekegn Zarihun (MSC.)Document55 pagesBasic Gymnastics: Tarekegn Zarihun (MSC.)Bayisa ShankoNo ratings yet
- Couch To 5K Jogging PlanDocument2 pagesCouch To 5K Jogging PlanByzantine PGNo ratings yet
- Poor 8 Pts Fair/ Below Average 10 Pts Good/Average 12 Pts Above Average 14 Pts Outstanding 16 PtsDocument3 pagesPoor 8 Pts Fair/ Below Average 10 Pts Good/Average 12 Pts Above Average 14 Pts Outstanding 16 PtsMaro Mempin-TabinasNo ratings yet
- Lesson 3: Training PrinciplesDocument24 pagesLesson 3: Training PrinciplesChen BalNo ratings yet