You might also like
- Typical Shoulder TroublesDocument7 pagesTypical Shoulder TroublesLev KalikaNo ratings yet
- Prevent Back InjuriesDocument22 pagesPrevent Back InjuriesSuganya Balachandran100% (1)
- 10Document25 pages10Sarthak GuptaNo ratings yet
- Comparison of Muscle Activation Using Various Hand Positions During The Push-Up ExerciseDocument6 pagesComparison of Muscle Activation Using Various Hand Positions During The Push-Up ExerciseJúnior Alvacir CamargoNo ratings yet
- Training - Principles - and - Methodscn (2) .PPT (Autosaved)Document48 pagesTraining - Principles - and - Methodscn (2) .PPT (Autosaved)EmmanuelNo ratings yet
- Tips On How To Improve Your Muscular Strength and EnduranceDocument9 pagesTips On How To Improve Your Muscular Strength and EnduranceAndy CRNo ratings yet
- Runner Muscular Balance Core Stability and Injury Prevention For Middle and Long Distance Runners PDFDocument21 pagesRunner Muscular Balance Core Stability and Injury Prevention For Middle and Long Distance Runners PDFAmmar ShamoutNo ratings yet
- 5 Strategies For Choosing ExercisesDocument5 pages5 Strategies For Choosing ExercisesFabianinhoLacerdaNo ratings yet
- Sports Training 4Document24 pagesSports Training 4simsa sin100% (1)
- ShoulderDocument36 pagesShoulderZuriman Abdul RahmanNo ratings yet
- Hip Application SolutionsDocument3 pagesHip Application SolutionsDNo ratings yet
- 360 MMRDocument11 pages360 MMRUriel Morales RodríguezNo ratings yet
- Resistance Exercise Chapter 6Document9 pagesResistance Exercise Chapter 6ambreenfatehNo ratings yet
- Movement ScreeningDocument12 pagesMovement ScreeningCláudio Milane De Oliveira100% (1)
- Stability: P. Ratan Khuman M.P.T. (Ortho & Sports)Document56 pagesStability: P. Ratan Khuman M.P.T. (Ortho & Sports)Diogo BarrosNo ratings yet
- Powerpoint Chapter 6-Student EditionDocument35 pagesPowerpoint Chapter 6-Student Editionbob poopersteinNo ratings yet
- Firstbeat Understanding Athlete Stress and Recovery 241018Document18 pagesFirstbeat Understanding Athlete Stress and Recovery 241018sashiNo ratings yet
- Shoulder Pain OverviewDocument37 pagesShoulder Pain Overvieweddie bechillNo ratings yet
- 5 Nutrition Mistakes Athletes MakeDocument3 pages5 Nutrition Mistakes Athletes MakeScott McLaneNo ratings yet
- Lower Crossed Syndrome - 6 Steps To Fix Anterior Pelvic Tilt and Swayback PostureDocument46 pagesLower Crossed Syndrome - 6 Steps To Fix Anterior Pelvic Tilt and Swayback Posturepujarze2No ratings yet
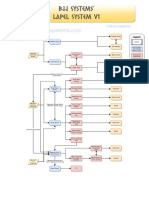
- BJJ Systems Lapel System A4 v1Document1 pageBJJ Systems Lapel System A4 v1Paniq UriosteguiNo ratings yet
- Office Ergonomics PowerpointDocument36 pagesOffice Ergonomics PowerpointBlanca PerezNo ratings yet
- Functional Training TorsoDocument2 pagesFunctional Training TorsoOtrovanjeNo ratings yet
- Plyometric Training Considerations To Reduce Knee.18 PDFDocument3 pagesPlyometric Training Considerations To Reduce Knee.18 PDFAndrew ShirekNo ratings yet
- Scapular Stabilizing Muscles Rehab ProtocolDocument2 pagesScapular Stabilizing Muscles Rehab ProtocolnimitrisNo ratings yet
- Understanding Postural Deformities Like KyphosisDocument36 pagesUnderstanding Postural Deformities Like KyphosisAashishRanjanNo ratings yet
- Improving PerformanceDocument18 pagesImproving Performanceapi-269691881No ratings yet
- Prehab GuysDocument4 pagesPrehab GuysEric SunNo ratings yet
- Core Muscle Strengthening in The AthleteDocument48 pagesCore Muscle Strengthening in The AthleteNicu Tanase-RaduNo ratings yet
- The Role of Core StabilityDocument11 pagesThe Role of Core StabilitykevintriyaNo ratings yet
- Nursing-AnaPhy-Muscular System Upper BodyDocument21 pagesNursing-AnaPhy-Muscular System Upper BodyGail Chantel Spring PerlasNo ratings yet
- Movement Skills - NEO BJJDocument9 pagesMovement Skills - NEO BJJVarto RazvanNo ratings yet
- Ankle Rehabilitation: DR - Zahoor Ahmad Assistant Professor NCS UniversityDocument25 pagesAnkle Rehabilitation: DR - Zahoor Ahmad Assistant Professor NCS UniversityZahoor AhmadNo ratings yet
- Upper Extremity Rom NormsDocument3 pagesUpper Extremity Rom Normsapi-336924644No ratings yet
- Rocktape Tactical Athlete Taping InstructionsDocument2 pagesRocktape Tactical Athlete Taping Instructionsdilligas1234No ratings yet
- Hip Flexor StrainDocument2 pagesHip Flexor StrainendurthiNo ratings yet
- Hamstring Injury - Diagnosis and Injury Management DiagnosisDocument5 pagesHamstring Injury - Diagnosis and Injury Management Diagnosisgemichan26No ratings yet
- Assessment and Examination of the ShoulderDocument31 pagesAssessment and Examination of the ShoulderNithin NairNo ratings yet
- Crossover Scaling Shoulder Guide 1Document6 pagesCrossover Scaling Shoulder Guide 1Alexandru SeciuNo ratings yet
- Balance Training Versus Balance Training and Foot and Ankle Mobilization A PilotDocument11 pagesBalance Training Versus Balance Training and Foot and Ankle Mobilization A Pilotmaria monicaNo ratings yet
- Knee Injuries Part 1Document38 pagesKnee Injuries Part 1meenoNo ratings yet
- What Do You All Think of Kneesovertoesguy - Are His Exercises Useful For Judokas in Your Opinions - JudoDocument3 pagesWhat Do You All Think of Kneesovertoesguy - Are His Exercises Useful For Judokas in Your Opinions - JudoAbbas RazaNo ratings yet
- Biomechanics of Hip 1Document19 pagesBiomechanics of Hip 1Muqeet76No ratings yet
- Animal FlowDocument1 pageAnimal FlowMadhab HalderNo ratings yet
- Strength Training For Karate Point Fighting-12.Week. Karate - Shotokan.kata - Kumite.kihon - Oliva.videDocument7 pagesStrength Training For Karate Point Fighting-12.Week. Karate - Shotokan.kata - Kumite.kihon - Oliva.videbodgieNo ratings yet
- 5 Myths About Eccentric Training Every Coach Ought To Know - SimpliFasterDocument1 page5 Myths About Eccentric Training Every Coach Ought To Know - SimpliFasterAyoub SELMINo ratings yet
- Warm Ups RAMPDocument19 pagesWarm Ups RAMPRichard Jerome Dela CruzNo ratings yet
- Lower Crossed SyndromeDocument8 pagesLower Crossed SyndromeThaseen75% (4)
- Acl Accelerated ProtocolDocument6 pagesAcl Accelerated ProtocolkapsicumadNo ratings yet
- Supraspinatus TendonitisDocument27 pagesSupraspinatus TendonitisnogenaziNo ratings yet
- Scapula DyskinesiaDocument5 pagesScapula Dyskinesiamiguelax1No ratings yet
- Gray Cook Self Limiting ExerciseDocument7 pagesGray Cook Self Limiting ExerciseWaldir Martins NetoNo ratings yet
- Rotator CuffDocument46 pagesRotator Cuffeuan00No ratings yet
- Driveline Drills Cheat SheetDocument1 pageDriveline Drills Cheat SheetJustin KilpatrickNo ratings yet
- Kinetic Chain Exercises - Open Versus ClosedDocument4 pagesKinetic Chain Exercises - Open Versus Closedamirreza jmNo ratings yet
- Aerobic & Anaerobic Exs: Dr. Meghan Phutane Cardiorespiratory PhysiotherapistDocument57 pagesAerobic & Anaerobic Exs: Dr. Meghan Phutane Cardiorespiratory PhysiotherapistNutrition ClinicNo ratings yet
- HSTWorkout PlannerDocument4 pagesHSTWorkout Plannerjohn lewisNo ratings yet
- Musculoskeletal Assessment Notes P CotterDocument55 pagesMusculoskeletal Assessment Notes P CotterHappy CherryNo ratings yet
- Knee Anatomy and InjuriesDocument120 pagesKnee Anatomy and Injurieserfan mohammadi100% (2)
- PE and Diagnosis of ElbowDocument58 pagesPE and Diagnosis of Elbowmupt77No ratings yet
- Skin Integrity and Wound CareDocument73 pagesSkin Integrity and Wound Caretj100% (1)
- Diabetes Risk Test Paper VersionDocument2 pagesDiabetes Risk Test Paper VersionThe Livingston County NewsNo ratings yet
- AsthmaDocument1 pageAsthmatjNo ratings yet
- Wong's Pediatric Nursing c28Document22 pagesWong's Pediatric Nursing c28tj100% (8)
- Realm of AngelsDocument9 pagesRealm of AngelsElisha100% (1)
- Cash Flow StatementDocument2 pagesCash Flow StatementEvy Nonita AnggusNo ratings yet
- Exploring Potentials of Leftovers Spaces Using Urban MetamorphosisDocument18 pagesExploring Potentials of Leftovers Spaces Using Urban MetamorphosisBiris GabrielNo ratings yet
- DSC MatDocument41 pagesDSC MatRamuCivilNo ratings yet
- Respiratory and Circulatory Systems Working TogetherDocument4 pagesRespiratory and Circulatory Systems Working TogetherShellane Blanco Sardua100% (1)
- Legal and Regulatory Environment of Business 17Th Edition Pagnattaro Solutions Manual Full Chapter PDFDocument36 pagesLegal and Regulatory Environment of Business 17Th Edition Pagnattaro Solutions Manual Full Chapter PDForlando.white207100% (12)
- CRMDocument32 pagesCRMJoel Dsouza100% (1)
- Ford Fiesta Workshop Manual 2011Document3,505 pagesFord Fiesta Workshop Manual 2011Silas Jorge89% (61)
- Chapter 2 Problems Working PapersDocument28 pagesChapter 2 Problems Working PapersZachLoving0% (1)
- G.R. No. 170192 DigestDocument2 pagesG.R. No. 170192 Digestjesryl sugoyanNo ratings yet
- Bayan Ko anthem of opposition to Aquino regimeDocument2 pagesBayan Ko anthem of opposition to Aquino regimemicaela vergara67% (3)
- ĐỀ 15Document7 pagesĐỀ 15DistressNo ratings yet
- Topic 1 - Introduction To HRDDocument16 pagesTopic 1 - Introduction To HRDHassan SallehNo ratings yet
- List of 400 English Synonyms & Antonyms - Practice To Beat Competition PDFDocument18 pagesList of 400 English Synonyms & Antonyms - Practice To Beat Competition PDFSaket SaxenaNo ratings yet
- James Et Al-2017-Earth Surface Processes and LandformsDocument20 pagesJames Et Al-2017-Earth Surface Processes and Landformsqwerrty1029384756No ratings yet
- 8.FULLER - Eight Ways To Fail To Make LawDocument8 pages8.FULLER - Eight Ways To Fail To Make Lawmeflaviola100% (2)
- Nutritional Value Functional Properties Industri Application of Fruit JuiceDocument11 pagesNutritional Value Functional Properties Industri Application of Fruit JuiceLSPRO LAMPUNGNo ratings yet
- Cir vs. GJM 202695Document1 pageCir vs. GJM 202695magenNo ratings yet
- Summary Covers Exam MaterialDocument30 pagesSummary Covers Exam MaterialWriting ServiceNo ratings yet
- Chapter 2-Meaning and Scope of Public FinanceDocument21 pagesChapter 2-Meaning and Scope of Public FinanceyebegashetNo ratings yet
- Australian Guidebook For Structural Engineers by Lonnie Pack 1138031852Document5 pagesAustralian Guidebook For Structural Engineers by Lonnie Pack 1138031852Frans ChandraNo ratings yet
- MUET Reading Task - Print OutDocument5 pagesMUET Reading Task - Print Out萱儿林No ratings yet
- DM - s2024 - 001 IMPLEMENTATION OF CATCH UP FRIDAYSDocument34 pagesDM - s2024 - 001 IMPLEMENTATION OF CATCH UP FRIDAYSJobelle Razon100% (34)
- SHS General Mathematics Q2 M7Document16 pagesSHS General Mathematics Q2 M7Abegail PanangNo ratings yet
- Jadwal Pemeliharaan Alat Medik ICUDocument28 pagesJadwal Pemeliharaan Alat Medik ICUsarifahaniNo ratings yet
- Engineering Prob & Stat Lecture Notes 6Document12 pagesEngineering Prob & Stat Lecture Notes 6EICQ/00154/2020 SAMUEL MWANGI RUKWARONo ratings yet
- Characteristics of Young Language LearnersDocument16 pagesCharacteristics of Young Language Learnersfatihgun007No ratings yet
- Scientific Theological Aspects of GeocentricityDocument222 pagesScientific Theological Aspects of GeocentricityAdi Dumitru100% (1)
- Robotics SeminarDocument17 pagesRobotics SeminarTejasvi PalNo ratings yet