You might also like
- 1 FINAL - Loong Sarcoma JSOF 29JUN19Document68 pages1 FINAL - Loong Sarcoma JSOF 29JUN19BarryNo ratings yet
- Abcess On The BackDocument17 pagesAbcess On The BackBarryNo ratings yet
- ID Ekspresi Cd44 Dan Aldh1 Penanda Sel PuncDocument9 pagesID Ekspresi Cd44 Dan Aldh1 Penanda Sel PuncRaedy SusantoNo ratings yet
- Abcess On The BackDocument17 pagesAbcess On The BackBarryNo ratings yet
- Abcess On The BackDocument17 pagesAbcess On The BackBarryNo ratings yet
- Luka 2 PDFDocument6 pagesLuka 2 PDFBarryNo ratings yet
- E383 Full PDFDocument11 pagesE383 Full PDFBarryNo ratings yet
- Phytohemagglutinin-Induced Mitotic Index in BloodDocument11 pagesPhytohemagglutinin-Induced Mitotic Index in BloodBarryNo ratings yet
- Betty 2018 IOP Conf. Ser.: Earth Environ. Sci. 125 012128Document6 pagesBetty 2018 IOP Conf. Ser.: Earth Environ. Sci. 125 012128BarryNo ratings yet
- TNBC Current PDFDocument36 pagesTNBC Current PDFBarryNo ratings yet
- TNBC PDFDocument25 pagesTNBC PDFBarryNo ratings yet
- DOD 14 February 2020Document1 pageDOD 14 February 2020BarryNo ratings yet
- Nihms 615599Document33 pagesNihms 615599Kurnia AnharNo ratings yet
- Betty 2018 IOP Conf. Ser.: Earth Environ. Sci. 125 012128Document6 pagesBetty 2018 IOP Conf. Ser.: Earth Environ. Sci. 125 012128BarryNo ratings yet
- Gastric Perforation 2Document4 pagesGastric Perforation 2BarryNo ratings yet
- Cureus 0011 00000003869Document6 pagesCureus 0011 00000003869BarryNo ratings yet
- Betty 2018 IOP Conf. Ser.: Earth Environ. Sci. 125 012128Document6 pagesBetty 2018 IOP Conf. Ser.: Earth Environ. Sci. 125 012128BarryNo ratings yet
- Neoajuvant KemoterapiDocument2 pagesNeoajuvant KemoterapiBarryNo ratings yet
- Ca ColonDocument49 pagesCa ColonBarryNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- OET Test 1 PA by DrNesma RabieDocument5 pagesOET Test 1 PA by DrNesma RabieRancesh FamoNo ratings yet
- McGrath MAC Video Laryngoscope Instructions For Use PDFDocument24 pagesMcGrath MAC Video Laryngoscope Instructions For Use PDFAnonymous MnaMZQWwCNo ratings yet
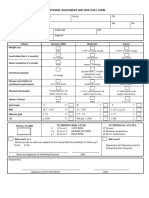
- 4 - Nutritional Assessment and Risk LevelDocument1 page4 - Nutritional Assessment and Risk LevelBok MatthewNo ratings yet
- Drug Free Pain Solution: Vibracool®Document8 pagesDrug Free Pain Solution: Vibracool®VUpendraNo ratings yet
- 10 1111@jocd 13505Document15 pages10 1111@jocd 13505Dr. Hilder HernandezNo ratings yet
- ICD 10 Codes For Dental Practice: L PracticesDocument9 pagesICD 10 Codes For Dental Practice: L PracticesAji HerlambangNo ratings yet
- NBC Part 7Document72 pagesNBC Part 7Shubham AggarwalNo ratings yet
- History: Develop An Illustrative Study of The Contributions of U.N.O. and It's Agencies - WHO, UNICHEF, UNESCODocument26 pagesHistory: Develop An Illustrative Study of The Contributions of U.N.O. and It's Agencies - WHO, UNICHEF, UNESCOAlfiya Khan0% (1)
- Spoliansky, Sara - Inglés Técnico TASK3Document3 pagesSpoliansky, Sara - Inglés Técnico TASK3Daniel SaúlNo ratings yet
- Health Policy and Technology: Weiwei Xu, Jing Wu, Lidan CaoDocument10 pagesHealth Policy and Technology: Weiwei Xu, Jing Wu, Lidan CaoArgonne Robert AblanqueNo ratings yet
- Physical Therapy AssessmentDocument38 pagesPhysical Therapy Assessmentnikki98% (56)
- You're Already: Le M Ge o M KneeDocument3 pagesYou're Already: Le M Ge o M KneeSara CoonNo ratings yet
- Journal On Self ConceptDocument6 pagesJournal On Self Conceptkspsridharan4899No ratings yet
- City Ordinance No.241: An Ordinance On Rabies Control and Eradication in Zamboanga CityDocument8 pagesCity Ordinance No.241: An Ordinance On Rabies Control and Eradication in Zamboanga CityArman BentainNo ratings yet
- Increasing Height 5 Tips To Grow Taller Even After Puberty The Times of IndiaDocument6 pagesIncreasing Height 5 Tips To Grow Taller Even After Puberty The Times of Indiawhite hatNo ratings yet
- Critical Care Intravenous Medications ChartDocument2 pagesCritical Care Intravenous Medications ChartMichelle Danielle MolinaNo ratings yet
- Basics of Mechanical VentilationDocument5 pagesBasics of Mechanical Ventilationruhaina malikNo ratings yet
- Lesson 5 - Review - Parts of The Body 1-2-3Document25 pagesLesson 5 - Review - Parts of The Body 1-2-3Alejandro GuerreroNo ratings yet
- Draft T& T LOLER RegulationsDocument68 pagesDraft T& T LOLER RegulationsDerron SoogrimNo ratings yet
- Eco Tex - Google Search PDFDocument1 pageEco Tex - Google Search PDFAbdul RaheemNo ratings yet
- Holistic Approach To Mental HealthDocument38 pagesHolistic Approach To Mental HealthabhishekNo ratings yet
- A Study On Air Pollution Tolerance Index (Apti) and Anticipated Performance Index (Api) of Some PlantsDocument9 pagesA Study On Air Pollution Tolerance Index (Apti) and Anticipated Performance Index (Api) of Some PlantsIJAR JOURNALNo ratings yet
- The French in North America Unit Chapter 2Document9 pagesThe French in North America Unit Chapter 2api-490517749No ratings yet
- Fire Your WifeDocument35 pagesFire Your Wifeonlineguy2449No ratings yet
- The Philosophy and Science of Caring Jean Watson: St. Luke'S College of Nursing Trinity University of AsiaDocument28 pagesThe Philosophy and Science of Caring Jean Watson: St. Luke'S College of Nursing Trinity University of Asiaojay_88No ratings yet
- Skin Cancer Detection Using Artificial Neural NetworkDocument24 pagesSkin Cancer Detection Using Artificial Neural NetworkShanu Shukla100% (1)
- Science Reviewer - FinaDocument3 pagesScience Reviewer - FinaAmamore Lorenzana PlazaNo ratings yet
- Radford High Athletic ComplexDocument27 pagesRadford High Athletic ComplexHNNNo ratings yet
- Kindeney Kharab Hone Ke LakchanDocument5 pagesKindeney Kharab Hone Ke Lakchanmydrive1980No ratings yet
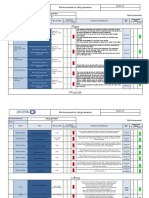
- Plant 6 3: Risk Assessment For Lifting OperationsDocument4 pagesPlant 6 3: Risk Assessment For Lifting OperationsIdris AdeniranNo ratings yet