You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Blood Bank Review 2019 PDFDocument613 pagesBlood Bank Review 2019 PDFCuddles Pingoy100% (1)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Effect of Squeezing On The Fingertip During Capillary Blood Collection To The Laboratory Analysis ResultsDocument8 pagesEffect of Squeezing On The Fingertip During Capillary Blood Collection To The Laboratory Analysis Resultsfardiah tilawatiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Essentials of Anatomy and PhysiologyDocument68 pagesEssentials of Anatomy and PhysiologyhamidiNo ratings yet
- Isoinmunizacion RH Actual ArticuloDocument11 pagesIsoinmunizacion RH Actual Articuloeloydc17No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Anemia NotesDocument8 pagesAnemia Notesalin malekNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Phlebotomy Chapt1Document19 pagesPhlebotomy Chapt1Mùkhtæær Ïbňü ÅhmēdNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Blood Grouping 12thDocument17 pagesBlood Grouping 12thPranjal SharmaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- FRM Patient View All ReportDocument6 pagesFRM Patient View All ReportShailesh KumarNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Case Studies - MIC3002Document28 pagesCase Studies - MIC300217206404 STUDENTNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- v02 NycoCard HbA1c - Package Insert - 1116112 - Re PDFDocument64 pagesv02 NycoCard HbA1c - Package Insert - 1116112 - Re PDFMariana VrvNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Vte Clinical Update Final - 190207 - 1 - LR FinalDocument6 pagesVte Clinical Update Final - 190207 - 1 - LR FinalSantosh SinghNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Quiz - Red Blood Cell and Bleeding Disorder - Attempt ReviewDocument78 pagesQuiz - Red Blood Cell and Bleeding Disorder - Attempt ReviewAdrian CaballesNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- bloodHT Exam QsDocument7 pagesbloodHT Exam QsPUNCHNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval ABO Group: RH Typing: MethodDocument1 pageLaboratory Test Report: Test Name Result Biological Reference Interval ABO Group: RH Typing: MethodPrathapuramnarasimhacharyuluNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Pemeriksaan DarahDocument11 pagesPemeriksaan DarahJems BoruNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- RH IncompatibilityDocument9 pagesRH IncompatibilityJohn BardeenNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Polycythemia Vera and Essential ThrombocythemiaDocument10 pagesPolycythemia Vera and Essential ThrombocythemiaNichole BrownNo ratings yet
- Lec.3 PhlebetomyDocument2 pagesLec.3 PhlebetomyQudamah JasemNo ratings yet
- Ifu - 771100 771101 en - 2017 12 19Document1 pageIfu - 771100 771101 en - 2017 12 19Khaled AlkhawaldehNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hematocrite Values With High Measurement of Eritrosit After Centrifugation On Serum MakingDocument10 pagesHematocrite Values With High Measurement of Eritrosit After Centrifugation On Serum MakingPutri Aswariyah RamliNo ratings yet
- Haematology 2018 Reading ListDocument2 pagesHaematology 2018 Reading ListnooneNo ratings yet
- Gel TechnologyDocument2 pagesGel TechnologyJai Carungay100% (1)
- Blood Transfusion and BloodDocument12 pagesBlood Transfusion and BloodAnusha AnanthakrishnaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Physiology Lab 2.1 Blood PhysiologyDocument8 pagesPhysiology Lab 2.1 Blood PhysiologyhellokrisjaejoongNo ratings yet
- Physiology Lab Report 2Document27 pagesPhysiology Lab Report 2Chuan RuiNo ratings yet
- المحاضرة 4Document5 pagesالمحاضرة 4Shi no MeNo ratings yet
- Hemoglobin MetabolismDocument4 pagesHemoglobin Metabolismrona hilarioNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
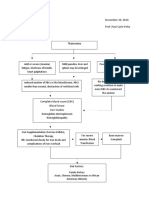
- Concept MapDocument2 pagesConcept MapcheskaotreraNo ratings yet
- Blood Transfusion Therapy DefinitionDocument27 pagesBlood Transfusion Therapy DefinitionEvangelin MelvinNo ratings yet
- CHECKLIST Blood TransfusionDocument7 pagesCHECKLIST Blood TransfusionBELIGANIO JOHANNANo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)