You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Module 5 Healthcare DeliverDocument64 pagesModule 5 Healthcare DeliverVelia PutriNo ratings yet
- Incident Reporting JciDocument14 pagesIncident Reporting Jciakinrav100% (2)
- Rad Tech CV ResumeDocument2 pagesRad Tech CV ResumeShiruzu Tomas GananshiruNo ratings yet
- Full Download Introduction To Health Care 4th Edition Mitchell Test Bank PDF Full ChapterDocument36 pagesFull Download Introduction To Health Care 4th Edition Mitchell Test Bank PDF Full Chapterhomelingcomposedvqve100% (18)
- Neuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcDocument7 pagesNeuropathic Orofacial Pain Patients in Need of Dental Care: Jcda JadcAlex GasnasNo ratings yet
- Suspected Neurological Conditions Recognition and Referral PDF 66141663923653Document76 pagesSuspected Neurological Conditions Recognition and Referral PDF 66141663923653Alex GasnasNo ratings yet
- Orofacial Pain - An Update On Diagnosis and Management: PracticeDocument9 pagesOrofacial Pain - An Update On Diagnosis and Management: PracticeAlex GasnasNo ratings yet
- Hypoglosal Nerve PalsyDocument4 pagesHypoglosal Nerve PalsyAlex GasnasNo ratings yet
- Facial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaDocument6 pagesFacial Pain: Neurological and Non-Neurological: Joanna M ZakrzewskaAlex GasnasNo ratings yet
- MITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorDocument25 pagesMITOCW - MIT9 - 00SCF11 - Lec20 - 300k.mp4: ProfessorAlex GasnasNo ratings yet
- 2150 FullDocument7 pages2150 FullAlex GasnasNo ratings yet
- Death PathologyDocument80 pagesDeath PathologyAlex GasnasNo ratings yet
- Freemasonry Uncovering FreemasonryDocument113 pagesFreemasonry Uncovering Freemasonrycigsas1719100% (1)
- Funke Et Al-2011-The Journal of PhysiologyDocument13 pagesFunke Et Al-2011-The Journal of PhysiologyAlex GasnasNo ratings yet
- "Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceDocument4 pages"Non-Invasive" Brain Stimulation Is Not Non-Invasive: Systems NeuroscienceAlex GasnasNo ratings yet
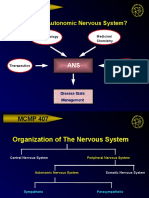
- MCMP 407: Why Study The Autonomic Nervous System?Document15 pagesMCMP 407: Why Study The Autonomic Nervous System?Alex GasnasNo ratings yet
- CNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaDocument70 pagesCNS Other Infections: Pediatric Critical Care Medicine Emory University Children's Healthcare of AtlantaAlex GasnasNo ratings yet
- Post-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraDocument7 pagesPost-Ischemic in Ammation in The Brain: Takashi Shichita, Ryota Sakaguchi, Mayu Suzuki and Akihiko YoshimuraAlex GasnasNo ratings yet
- Application For The Approval of Project ProposalDocument11 pagesApplication For The Approval of Project ProposalSanjeev ChouguleNo ratings yet
- Man Up A Practical Guide For Men in NursingDocument263 pagesMan Up A Practical Guide For Men in NursingAjep TohajudinNo ratings yet
- Patient SafetyDocument258 pagesPatient SafetycosommakNo ratings yet
- Business ManDocument6 pagesBusiness MannishantNo ratings yet
- JCI Newsletter May 8 IPSGDocument6 pagesJCI Newsletter May 8 IPSGAhmad HaririNo ratings yet
- PSATDocument578 pagesPSATDubey Deepak100% (1)
- Apollo Gleneagles HospitalsDocument23 pagesApollo Gleneagles Hospitalssujal verma100% (1)
- 2011 Fall JCR International CatalogueDocument32 pages2011 Fall JCR International CatalogueJoao HeckerNo ratings yet
- ApolloDocument82 pagesApolloRaj KumarNo ratings yet
- Lauren B. LittlejohnDocument16 pagesLauren B. Littlejohnapi-516216369No ratings yet
- Congress CPDocument143 pagesCongress CPazay101No ratings yet
- Shawa - Patients Perceptions Regarding Nursing Care in The General Surgical Wards at Kenyatta National Hospital - NinisannnDocument103 pagesShawa - Patients Perceptions Regarding Nursing Care in The General Surgical Wards at Kenyatta National Hospital - Ninisannnnoronisa talusobNo ratings yet
- Public Health TerminologyDocument17 pagesPublic Health Terminologymohammed RAFINo ratings yet
- Alcohol Treatment Facility Business Plan FY-02Document7 pagesAlcohol Treatment Facility Business Plan FY-02Keith BeckerNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument11 pagesMedical Devices Inspection and Maintenance A Literature ReviewAarsol AdvanceNo ratings yet
- ccpc15 Practice Administration and Development Protocol Development WorkbookDocument26 pagesccpc15 Practice Administration and Development Protocol Development WorkbookJeremy HamptonNo ratings yet
- Terminology, Abbreviations and Symbols Used in The Prescribing and Administration of MedicinesDocument8 pagesTerminology, Abbreviations and Symbols Used in The Prescribing and Administration of MedicinesMia MihaelaNo ratings yet
- Quality AssuranceDocument23 pagesQuality AssuranceswethashakiNo ratings yet
- My Final ReportDocument78 pagesMy Final ReportjhutayNo ratings yet
- Foreword Acknowledgements: IFC Self-Assessment Guide For Health Care OrganizationsDocument16 pagesForeword Acknowledgements: IFC Self-Assessment Guide For Health Care OrganizationsYL LYNo ratings yet
- IlsmDocument21 pagesIlsmIcaza IcazaNo ratings yet
- Chapter 02 PDFDocument9 pagesChapter 02 PDFMartha TreviñoNo ratings yet
- Emergency Drills ExercisesDocument28 pagesEmergency Drills ExercisesZawawi Ibnu RosyidNo ratings yet
- Focused and Ongoing Professional Practice EvaluationsDocument29 pagesFocused and Ongoing Professional Practice EvaluationsDwi cahyaniNo ratings yet
- Web SitesDocument41 pagesWeb Sitesเกมกวี MedicalStudentNo ratings yet
- Eoc Risk Assessment Jci-1 PDFDocument136 pagesEoc Risk Assessment Jci-1 PDFYulanda SeptaNo ratings yet