You might also like
- Chapter Four: - Assessments of CommunityDocument37 pagesChapter Four: - Assessments of CommunityAbdurohaman BelayNo ratings yet
- Concept of Community NutritionDocument4 pagesConcept of Community NutritionNrs Sani Sule MashiNo ratings yet
- Community NutritionDocument22 pagesCommunity NutritionLilis IndriNo ratings yet
- Diet Survey (SUKRITI)Document37 pagesDiet Survey (SUKRITI)Juhi Neogi100% (1)
- Nutritional Deficiency For ClassDocument74 pagesNutritional Deficiency For ClassBelayneh TadesseNo ratings yet
- 1 Script200302090903033030Document9 pages1 Script200302090903033030gever29816No ratings yet
- Underweight and MalnutritionDocument61 pagesUnderweight and MalnutritionJack Sinaga100% (1)
- Nutritional Surveillance ModuleDocument57 pagesNutritional Surveillance ModuleDwi Ayu Lestari100% (1)
- Nutritional AssessmentDocument49 pagesNutritional AssessmentIrene Grace Balcueva100% (1)
- CHAPTER 1 Introduction To Community Nutrition PDFDocument24 pagesCHAPTER 1 Introduction To Community Nutrition PDFZzati Fida'iyNo ratings yet
- Nutritional AssessmentDocument45 pagesNutritional AssessmentWondimu EliasNo ratings yet
- The Factors That Influence Our Food Choices: 1. Major Determinants of Food ChoiceDocument18 pagesThe Factors That Influence Our Food Choices: 1. Major Determinants of Food ChoiceFrancis GongNo ratings yet
- Community Nutrition ProgrammeDocument27 pagesCommunity Nutrition Programmeprabha krishnan100% (4)
- Nutritional Status AssessmentDocument38 pagesNutritional Status Assessmentmichael jan de celis100% (3)
- NUTRITION IN EMERGENCIES Full Notes-1Document34 pagesNUTRITION IN EMERGENCIES Full Notes-1Donvan Nunda100% (1)
- Community NutritionDocument297 pagesCommunity NutritionSaba SharifNo ratings yet
- Individual, Family, Community As A Unit of Health ServiceDocument10 pagesIndividual, Family, Community As A Unit of Health ServiceNeha Verma50% (2)
- Dietary Assessment Methods in Nutrition EpidemiologyDocument14 pagesDietary Assessment Methods in Nutrition EpidemiologyArMadea De'aMraNo ratings yet
- Determinants of HealthDocument30 pagesDeterminants of HealthRuchi YadavNo ratings yet
- Nutritional Needs of AdolescentsDocument9 pagesNutritional Needs of AdolescentsLstr B PrltaNo ratings yet
- Nutrition Course For PHO Dec, 2022Document142 pagesNutrition Course For PHO Dec, 2022Semon YohannesNo ratings yet
- Therapeutic DietDocument19 pagesTherapeutic DietJenny Rose Aniete67% (3)
- Community NutritionDocument13 pagesCommunity NutritionVaishali Jainarain100% (2)
- Nutritional SurveillanceDocument20 pagesNutritional SurveillanceWakjira GemedaNo ratings yet
- A Balanced DietDocument11 pagesA Balanced Dietaliciamargaretha100% (2)
- Community Health Nursing Lab Helps Develop Knowledge, AttitudesDocument1 pageCommunity Health Nursing Lab Helps Develop Knowledge, AttitudesChakrapani Chaturvedi100% (1)
- Nutri Lect1-6Document68 pagesNutri Lect1-6Zharm MayNo ratings yet
- NURSING CODE OF ETHICSDocument12 pagesNURSING CODE OF ETHICSCol Vijayan100% (1)
- Lec - 9 Public Health Nutrition and Importance For Health PromptionDocument44 pagesLec - 9 Public Health Nutrition and Importance For Health Promptiontanvir ahmed0% (1)
- Information Communication EducationDocument19 pagesInformation Communication EducationNarjina Begam100% (1)
- Demography and Family Planning: Community Health Nursing Unit IIDocument49 pagesDemography and Family Planning: Community Health Nursing Unit IIramita sahNo ratings yet
- 4 Nutritional AssessmentDocument42 pages4 Nutritional AssessmentChinju Cyril100% (1)
- Assessment of Nutritional SituationDocument24 pagesAssessment of Nutritional SituationMawasumi Ayu Andini0% (1)
- 1.1 Introduction To Nutrition, Nutrient Needs, Nutrition Tools, Food ChoicesDocument94 pages1.1 Introduction To Nutrition, Nutrient Needs, Nutrition Tools, Food Choicesjunelyn ong100% (1)
- Recommendations of Various Health CommitteesDocument27 pagesRecommendations of Various Health CommitteesHimanshu Chauhan100% (2)
- Unit - XI-Role of Nurse in Nutrition ProgrammeDocument82 pagesUnit - XI-Role of Nurse in Nutrition ProgrammeEllen AngelNo ratings yet
- Community DiagnosisDocument44 pagesCommunity DiagnosisMenuka Shrestha100% (3)
- IGNOU Block 2 Unit 5 Foodborne Diseases and Food SafetyDocument26 pagesIGNOU Block 2 Unit 5 Foodborne Diseases and Food Safetyerice.researchNo ratings yet
- Basic Measures of EpidemiologyDocument51 pagesBasic Measures of EpidemiologyHafiz SabghatullahNo ratings yet
- Community NuitritionDocument12 pagesCommunity Nuitritionmariet abrahamNo ratings yet
- CPHN Long ExamDocument13 pagesCPHN Long ExamJohn Michael MacabentaNo ratings yet
- Ecology of MalnutritionDocument10 pagesEcology of MalnutritionnareshraopendyalaNo ratings yet
- Determination of Energy Value of Foods Using Bomb and Indirect CalorimetryDocument18 pagesDetermination of Energy Value of Foods Using Bomb and Indirect CalorimetryANJALI100% (1)
- Primary Health CareDocument41 pagesPrimary Health CareKailash NagarNo ratings yet
- 6 Nutritional InterventionDocument33 pages6 Nutritional InterventionNegeso JaraNo ratings yet
- Rajiv Gandhi University of Health Sciences, Karnataka, BangaloreDocument18 pagesRajiv Gandhi University of Health Sciences, Karnataka, Bangaloreabdullah khalidNo ratings yet
- Food AdulterationDocument13 pagesFood Adulterationramanjeet kaurNo ratings yet
- Nutritional AssessmentDocument16 pagesNutritional AssessmentGelo Libelo100% (1)
- Fundamentals of Nursing-Meeting Basic Client Nutritional NeedsDocument31 pagesFundamentals of Nursing-Meeting Basic Client Nutritional NeedsManasseh Mvula77% (13)
- HEALTH EDUCATION GUIDEDocument84 pagesHEALTH EDUCATION GUIDEJesus Mario Lopez100% (2)
- Diet & Nutrition CounsellingDocument7 pagesDiet & Nutrition Counsellingshilpasheetal0% (1)
- Health Education - Intro, Aims & ScopeDocument18 pagesHealth Education - Intro, Aims & Scopeanwaralimalikstar67% (6)
- Community Nutrition: Prepared By:Mrs Bemina J A Assistant Professor ESIC College of Nursing KalaburagiDocument52 pagesCommunity Nutrition: Prepared By:Mrs Bemina J A Assistant Professor ESIC College of Nursing Kalaburagibemina ja100% (1)
- Lecture 10 Protein Energy Malnutrition (PEM)Document26 pagesLecture 10 Protein Energy Malnutrition (PEM)jaish8904100% (1)
- Case Study - NutritionDocument10 pagesCase Study - NutritionJ.SNo ratings yet
- Health CommitteeDocument35 pagesHealth CommitteeshailaNo ratings yet
- Health Education MethodsDocument16 pagesHealth Education Methodsfabiopira183% (12)
- Health Promotion (Eng)Document25 pagesHealth Promotion (Eng)JaneLorensNo ratings yet
- Canadian Undergraduate Urology Curriculum (CanUUC): Urinary Calculus DiseaseDocument47 pagesCanadian Undergraduate Urology Curriculum (CanUUC): Urinary Calculus DiseaseNizwan ShamNo ratings yet
- Lab Normal Values ReferenceDocument4 pagesLab Normal Values ReferenceMuhammad Fikru RizalNo ratings yet
- Environmental Health: Introduction ofDocument54 pagesEnvironmental Health: Introduction ofNizwan ShamNo ratings yet
- Malaysian Society of Anaesthesiologists College of Emergency Physicians, AMM College of Anaesthesiologists, AMM Academy of Medicine of MalaysiaDocument22 pagesMalaysian Society of Anaesthesiologists College of Emergency Physicians, AMM College of Anaesthesiologists, AMM Academy of Medicine of MalaysiabapaknyanadlirNo ratings yet
- AsthmaDocument142 pagesAsthmaAmirah Mohamad Saidi100% (1)
- Tumour Lysis Syndrome & Fe Brile Neutropenia: Supervisor: DR Asmidar Prepared By: Nizwan, Hajar, DorothyDocument38 pagesTumour Lysis Syndrome & Fe Brile Neutropenia: Supervisor: DR Asmidar Prepared By: Nizwan, Hajar, DorothyNizwan ShamNo ratings yet
- QR Management of Ischaemic Stroke (2nd Edition) PDFDocument20 pagesQR Management of Ischaemic Stroke (2nd Edition) PDFAzizan HannyNo ratings yet
- CPG Management of Ischaemic Stroke (2nd Edition) PDFDocument64 pagesCPG Management of Ischaemic Stroke (2nd Edition) PDFPrince o'Spirit o'Soul ChaiNo ratings yet
- ED Topics HODocument2 pagesED Topics HONizwan ShamNo ratings yet
- NAG 19 UnlockedDocument290 pagesNAG 19 UnlockedncyNo ratings yet
- ED Topics HODocument2 pagesED Topics HONizwan ShamNo ratings yet
- Thaiger Thailand's News and Information SourceDocument1 pageThaiger Thailand's News and Information SourceWalailak PonlawatNo ratings yet
- Data Peserta & BusDocument10 pagesData Peserta & Busl24pkckembanganNo ratings yet
- Guardian Angel - Cara MaloneDocument177 pagesGuardian Angel - Cara MalonenoNo ratings yet
- Medico Legal Report - ThamaeDocument13 pagesMedico Legal Report - ThamaencetaniNo ratings yet
- ABYIPDocument4 pagesABYIPVi VianneNo ratings yet
- Ip 242 - 83-Schoniger Oxygen Flask Method PDFDocument3 pagesIp 242 - 83-Schoniger Oxygen Flask Method PDFPedro AluaNo ratings yet
- Gram Negative CocciDocument14 pagesGram Negative CocciRachel Marie M. GaniaNo ratings yet
- STD Risk Assessment QuestionnaireDocument1 pageSTD Risk Assessment QuestionnaireTine GuibaoNo ratings yet
- Scott Cunningham - Cunningham's Encyclopedia of Wicca in The KitchenDocument6 pagesScott Cunningham - Cunningham's Encyclopedia of Wicca in The KitchenPandora Storm0% (1)
- Full Report Wastewater Paling Latest BiaDocument44 pagesFull Report Wastewater Paling Latest BiaSyazwi HakimiNo ratings yet
- Sterilization of Operation Theatres - Time To Stop FumigationDocument2 pagesSterilization of Operation Theatres - Time To Stop Fumigationtummalapalli venkateswara rao100% (1)
- Pre AnestesiDocument64 pagesPre AnestesiKevin YonathanNo ratings yet
- 1.05 Liver and Portal HypertensionDocument12 pages1.05 Liver and Portal HypertensionZazaNo ratings yet
- BronchitisDocument22 pagesBronchitisEvita AdiningtyasNo ratings yet
- Gima CatalogDocument84 pagesGima Catalogsara şovreNo ratings yet
- 05-OSH Promotion Training & CommunicationDocument38 pages05-OSH Promotion Training & Communicationbuggs115250% (2)
- Biomechanics of the Lower ExtremitiesDocument17 pagesBiomechanics of the Lower ExtremitiesMilind GuptaNo ratings yet
- Human Resource Management: Safety, Health, and Risk ManagementDocument28 pagesHuman Resource Management: Safety, Health, and Risk ManagementA.s.qudah QudahNo ratings yet
- Breathing Pattern Assessment and InterventionDocument3 pagesBreathing Pattern Assessment and InterventionAziil LiizaNo ratings yet
- PROGRESS TEST 7 REVIEWDocument3 pagesPROGRESS TEST 7 REVIEWadevoicuNo ratings yet
- Mental Health and WellbeingDocument5 pagesMental Health and WellbeingNicole Ofili100% (1)
- How To Ensure Safety For Castable MixingDocument4 pagesHow To Ensure Safety For Castable MixingNaelNo ratings yet
- Journal of Trace Elements in Medicine and Biology: NutritionDocument8 pagesJournal of Trace Elements in Medicine and Biology: NutritionCamilla AndreatoNo ratings yet
- Challenges Implementing Telemedicine in AfghanistanDocument6 pagesChallenges Implementing Telemedicine in AfghanistanMuhibullah AmanNo ratings yet
- Case History EndodonticsDocument1 pageCase History EndodonticsDurva JainNo ratings yet
- Weebly Professional Development Plan FeedbackDocument3 pagesWeebly Professional Development Plan Feedbackapi-241839714No ratings yet
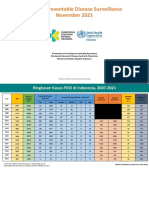
- 11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Document57 pages11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Kiky RizkyNo ratings yet
- Consanguinity Tulyagotriya Vivaha Impact On Child Health A Review LiteratureDocument4 pagesConsanguinity Tulyagotriya Vivaha Impact On Child Health A Review LiteratureEditor IJTSRDNo ratings yet
- Pestal Analysis of Pharmaceutical IndustryDocument12 pagesPestal Analysis of Pharmaceutical IndustrynaviguguNo ratings yet
- Chapter-4: Programme of Law Reform (1999) Pp. 18 and 43Document72 pagesChapter-4: Programme of Law Reform (1999) Pp. 18 and 43Humanyu KabeerNo ratings yet